Basal Ganglia in a neuroanatomy and a neurophysiology viewpoint
The Basal Ganglia consists of 5 large subcortical nuclei that participate in the control of movement, but do NOT have either direct input or output with the spinal cord; rather, they interact with the prefrontal and premotor cortices and therefore influence the planning and initiation of movements. In addition, the basal ganglia is involved in cognitive functions and behaviors unrelated to movement.
Definition:
1. Basal ganglia: corpus striatum, amygdala, and claustrum (anatomical).
2. Basal ganglia: corpus striatum, substantia nigra, and subthalamic nucleus (clinical)
3. Corpus striatum: caudate nucleus, lentiform nucleus (putamen+ globus pallidus)
4. Neostriatum (striatum)= caudate nucleus and putamen
5. Paleostraitum (pallidum) = globus pallidus
Anatomy:
1. Caudate nucleus: located between lateral ventricle and internal
capsule(follow contour of lateral ventricle)
2. Putamen: between external capsule and globus pallidus, deep to insular cortex( for visceral and taste function )
3. Globus pallidus: medial to putamen. divided into medial and lateral segments.
4. Substantia nigra: located dorsal to crus cerebri in the midbrain. divided in to pars compacta( uses dopamine), and pars reticulata( uses GABA)
5. Subthalamic Nucleus: oval shaped area in subthalamic region. Receiving information from Globus pallidus lateral segment, and sending output to globus pallidus medial segment and substantia nigra pars reticulata via glutamate neurotransmitter.

Clinical relationships:
General pathway: entire cerebral cortex → striatum → form circuitry with intrinsic nuclei ( globus pallidus lateral, SNc, ST), through output nuclei (globus pallidus medial, and SNr) → to VL, VM of thalamus (stimulate "+" or inhibit" -") → the prefrontal and premotor area of cortices.

Lesion may cause movement disorders, NOT paralysis. The disorders can be divided into hyperkinesias or hypokinesias.
-
Hyperkinesias: Lesions remove a controlling influence on motor cells in the cortex and produce hyperactivity involving involuntary, purposeless movements on the contralateral side.
a. athetosis- slow, writting, worm-like movements; aimless; involves the extremities, face, and neck. may be associated with cerebral palsy.
b. chorea- brisk, irregular, involuntary movements. pronounced in trunk, limb, and facial muscles.
c. hemiballismus- uncontrollable succession of violent movements of large areas of the body;
-
Hypokinesia: slow, absence of, or difficulty in starting/ stopping movements
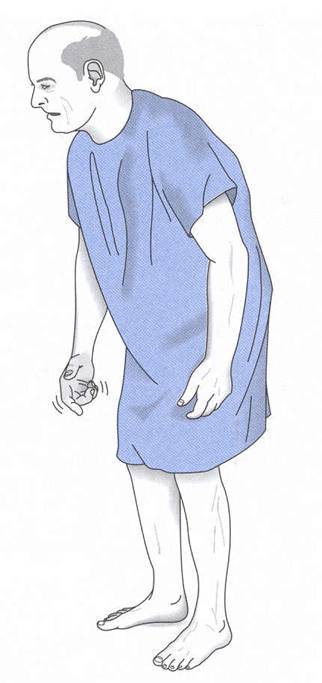
Example: Parkinson's disease- lose of substance nigra( which can decrease dopamine). You will see tremor at rest, rigidity, and bradykinesia(extreme slowness of movement).
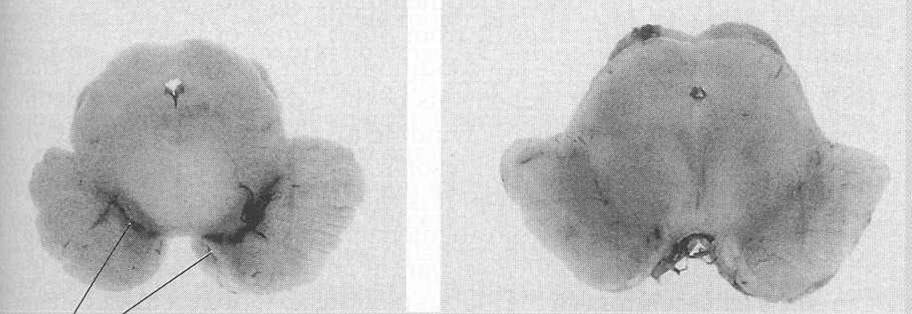
 you
can see loss of substantia nigra. You can also see the deposit of lewy
bodies in Parkinson's disease patient.
you
can see loss of substantia nigra. You can also see the deposit of lewy
bodies in Parkinson's disease patient.
References:
Murray L. Barr, John A. Kiernan: The Human Nervous System 6th edition, J.B. Lippincot Company 1993
Duane E. Haines: Neuroanatomy- An atlas of structures, sections, and systems 4th ed, Williams & Wilkins 1995
Eric R. Kandel: Principles of neural science 3rd ed, Appleton & Lange 1991