|
THE
EFFECT OF “LAGUNDI”( a local herb) TABLETS ON By: Romeo P. Chu, M.D. **
Forty otherwise asthmatics were included in a randomized double-blind comparative study between lagundi tablets and the standard drug theophylline. There were 20 subjects per treatment group; 7 of the subjects were males and 33 females. The patient profiles of both treatment groups were comparable. Likewise, the baseline parameters of both groups were also comparable. Results showed that both Lagundi and Theophylline caused significant bronchodilation over time. Statistical analysis showed significant increase in the mean peak expiratory flow rate (PEFR) of the lagundi group beginning at the 3rd hour. This shows the onset of action of lagundi to be at 3 hours post dosing. For the theophylline group, significant increase in the PEFR values was noted at 1 hour which corresponds to its onset of action. ANOVA with repeated measures showed no significant difference between lagundi and theophylline with respect to their effects on PEFR. However, since the sample size is inadequate, it cannot yet be concluded that lagundi is as effective as theophylline. Patients treated with lagundi failed to show a significant improvement of their wheezing over time but might have prevented the wheezing from getting worse. Patients treated with theophylline however, showed significant improvement of their wheezing as early as the 2nd hour. The theophylline treated patients had significantly better wheezing scores then the lagundi group at the 6th, 8th, 24th and 48th hour. There were no significant difference in the severity of the cough, dyspnea and chest pain in both treatment groups over time. However, the theophylline treated group had better “cough” than the “lagundi” group at the 24th and 48th hour. The theophylline group also had better “dyspnea” scores than the lagundi group at the 48th hour. There was no significant difference between lagundi and theophylline in terms of the effects on pulse rate (PR), respiratory rate (RR), and blood pressure (BP) readings. However, there was significant decrease in the mean sitting systolic BP and standing diastolic BP over time. This needs further investigation. Side effects reported in the lagundi group were vomiting, desquamation of the skin over the palms and increased urination. In the theophylline group, the side effects reported were nausea, vomiting, cold sweats, palpitation, tremors, headache and epigastric pain. Overall, lagundi displayed significant bronchodilating effects. Although theophylline has a slight edge in terms of therapeutic efficacy, lagundi still holds to be a promising drug in the future.
1. To determine the therapeutic
efficacy of lagundi tablets on bronchial asthma
in adults; METHODOLOGY: A. Preparation of Test
Drugs
a. Males and females 14
years and above with definite history of asthma The patient’s peak
expiratory flow rate is recorded before and 15 minutes after 2 inhalations
of a metered dose (100 mcg) of salbutamol aerosol. Only patients whose
PEFR is increased by 20% will be admitted to the study. 2. Exclusion Criteria: C. Study Design After a patient has been
selected as a candidate for the study and has given informed consent,
the following procedures were performed: In
all patients enrolled in the study, sufficient time was allowed for
recovery from the salbutamol test (at least 8 hours). Once the PEFR
is again less then 85%, than the study is resumed. Side effects or adverse reactions were described and properly recorded. D. Intercurrent Events Patients were not allowed to take concomitant medications during the study. If the patient does not respond to either lagundi or theophylline, then salbutamol tablets at a maximum dose of 2 mg every 8 hours will be added to the regimen and recorded.
Analysis of variance (ANOVA) with repeated observations with respect to time was used for data on theophylline and lagundi dosed for the four variables: blood pressure, pulse rate, respiratory rate and PEFR. If a statistically significant result is obtained, Duncan Multiple Range Test was employed to determine the specific periods of observation which are significantly different from baseline. Friedman Two Way analysis of variance was employed to determine if there was significant difference in the severity of cough, wheezing, dyspnea and chest pain over time. Mann-Whitney U test was used to determine if there was significant difference between the two treatment groups with respect to their effect on the severity of wheezing, cough, dyspnea and chest pain.
From
Sept 22 to
The 40 subjects
were equally distributed for each treatment group—20 in the lagundi
group and 20 in the theophylline group. There were 7 males and 33 females
with a ratio of 1:4.7. In the lagundi group, there were 19 females and
only 1male, while in the theophylline group; there were 14 females and
6 males.
All blood
chemistries were well within normal limits except for 2 patients. One
of these is in the lagundi group and has a WBC count of 13,000/mm3.
The other patient is in the theophylline group and has a WBC count of
10,000/ mm3. Both have normal differential counts and had no clinical
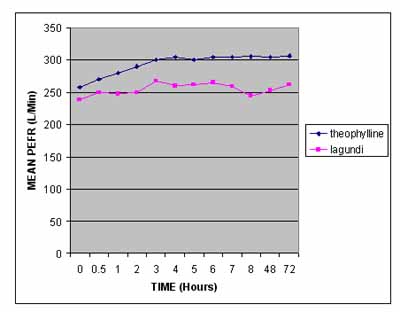
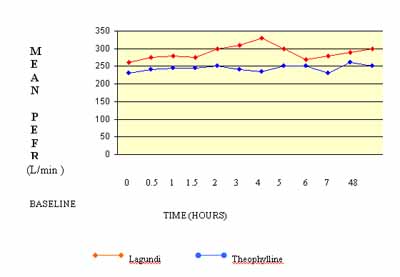
evidence of infection. 25 out of the 40 subjects had their chest x-ray done within the year. All showed normal findings except for 4 patients. 2 showed minimal infiltrates in the upper lung fields interpreted as minimal pulmonary tuberculosis activity undetermined. One of these belong to the lagundi group while the other to the theophylline group. One of the patients in the lagundi group had a chest x-ray which showed emphysematous changes while the other patient in the theophylline group showed streaky densities in the lower lung fields interpreted as chronic non-specific inflammatory disease. Figure 1 illustrates graphically the mean PEFR values of both the lagundi and theophylline treated groups over time. The ANOVA repeated measures showed a significant difference in the mean PEFR values of both the treated groups over time. This means that both drugs, lagundi and theophylline, caused significant bronchodilation over time. Comparing the 2 drugs in terms of their effect on the PEFR values using the ANOVA with repeated measures, the result showed no significant difference between the 2 treatment groups at P>0.05. However, since the sample size is still inadequate, it cannot yet be concluded that lagundi is as effective as theophylline. Figure 2 illustrates graphically the mean pulse rate of both treatment groups over time. ANOVA with repeated measures showed no significant difference in the pulse rate of both treatment groups over time. This means that both drugs are safe and that they do not significantly affect the pulse rate. They are neither myocardial stimulants nor depressants. There was
also no significant difference between the 2 groups in terms of their
effect on the pulse rate. Figure 4 illustrates graphically the mean sitting blood pressure (BP) of both the treatment groups over time. There was significant difference in the mean sitting systolic BP over time for both treatment groups. In the lagundi group, the mean baseline systolic BP at sitting position was 109.75 mmHg. At 30 mins and at the 6th hour, this was significantly lower at 30 mins with a mean reading of 106.9 mmHg. This was also noted at the following observation periods: 2 hrs, 4 hrs, 5 hrs, 6hrs, 8 hrs and 72 hrs. These changes could be due to the fact that the patients were rested for a longer period of time. It is also important to note that although there was a significant decrease in the sitting systolic BP, this effect was not consistent throughout the study periods. No patient reached hypotensive levels nor were there complaints of dizziness attributable to the decline in BP. All these plus the fact that all patients (except for the 2 previously mentioned hypertensives) were normotensive seem to point out that these differences were not really that important. These findings were also not consistent with the 2 patients (both in the lagundi group) with mild hypertension. One patient had a slight increase in systolic BP while the other had a slight decrease. Comparing the two, there was no significant difference between the lagundi and theophylline in terms of their effect on the sitting systolic BP. For the sitting diastolic BP, there was no significant difference in the 2 treatment groups over time. There was no significant difference between the 2 groups in terms of their effect on the sitting diastolic BP. Figure 5 illustrates graphically the mean standing BP readings of both treatment groups over time. ANOVA with repeated measurements showed no significant difference in standing systolic BP of both groups over time. There was also no significant difference between the two groups in terms of their effects on the standing systolic BP. There was significant difference in the mean standing diastolic BP for both treatment groups over time. For the lagundi group, the baseline mean diastolic BP in standing position was 84 mmHg and there was a significant decrease to 77 mmHg noted at the 4th hour up to the 8th hour and at the 24th hour. For the theophylline group, the baseline mean standing diastolic BP was 79.8 mmHg which significantly decreased to 75 mmHg at 30 mins. , the first hour and the 4th hour. Again, the reason previously cited could be used to explain the significant decrease in the BP readings, i.e. – relief of bronchospasm and longer period of rest. Similarly, the significant decrease was not persistent throughout the study period and the patients did not reach hypotensive levels.
The study shows that in the severity score for wheezing in the lagundi group over time, the higher the rank sum, the more severe is the wheezing. Note that the changes in the scores are minimal. Using the Friedman 2 way ANOVA, there is no significant difference in the severity of wheezing at P>0.05. This means that patients treated with lagundi failed to show significant improvement of their wheezing over time but might also mean that lagundi prevented their wheezing from getting worse. The severity scores for wheezing in the theophylline group over time showed results of statistical analysis indicating significant improvement in the severity of wheezing at P>0.05. This was noted as early as the second hour and was sustained throughout the study period. Mann Whitney U test was utilized to compare the 2 treatment groups with respect to their effects on wheezing. There was a significant difference between the 2 treatment groups noted at the 6th, 8th, 24th and 48th hours. This means that the improvement in the severity of wheezing in the theophylline group was significantly better than the lagundi group at the observation period stated above.
Statistical analysis of the severity scores for cough in the lagundi group over time showed no significant difference in the severity of cough in this treatment group at P>0.05. This means that patients treated with lagundi failed to show significant improvement or deterioration of their cough over time. A larger sample size might be able to detect a significant difference. Although previous studies showed lagundi to be effective against cough of viral origin, the parameter used was more of frequency rather than severity, so the results are not quite comparable. Statistical analysis of the severity scores in the theophylline treated group over time also showed no significant difference in the severity of cough in this treatment group over time at p>0.05. Although theophylline afforded significant relief of the bronchospasm and improvement of wheezing, there is still no significant improvement of its associated cough. A larger sample size might be able to detect a significant difference. Comparing the two treatment groups with respect to their effects on cough, there is a statistically significant difference between the lagundi group and the theophylline group at the 24th and 48th hour. This means that the improvement of cough in the theophylline treated group was significantly better than the lagundi treated group at the above stated observation periods. Dyspnea Statistical analysis of the severity scores for dyspnea in the lagundi treated group showed no significant difference in the severity of dyspnea in this treatment group over time at p>0.05. This means that although patients treated with lagundi had significant relief of their bronchospasm, there was no significant improvement in the severity of their dyspnea. However, lagundi might have prevented them from getting worse. With regards
to the severity scores of dyspnea in the theophylline treated group
over time, statistical analysis showed no significant difference in
the severity of dyspnea in this treatment group over time at p>0.05.
This means that the degree of dyspnea in patients treated with theophylline
neither improved nor worsened.
Friedman 2 way ANOVA showed no significant difference in the severity of chest pains overtime for the lagundi group at p>0.05. This means that patients treated with lagundi failed to show a significant improvement or worsening of their chest pains over time. For the severity scores for chest pain in the theophylline group over time, statistical analysis showed no significant difference in the severity of chest pain over time for this treatment group at p>0.05. This means that patients treated with theophylline failed to show a significant improvement or worsening of their chest pain over time. Comparing the two treatment groups with respect to their effect on chest pain, there is no significant difference between the lagundi and theophylline group at any observation period. Not one drug is superior over the other with respect to their effect on chest pain.
12 patients (30% of the sample size) took salbutamol tablets after 24 hrs because they developed asthmatic attacks. Eight were in the lagundi group and four were in the theophylline group. Of the 8 patients in the lagundi group, one patient took 8 salbutamol tablets (this patient had been on prednisone for 10 days but has stopped since 3 weeks prior to the study and had fair control of her asthma. Her bronchial airway hyperactivity might have flared up again); one patient took 4 tablets; another took 2 tablets and 3 patients took 1 tablet each. The total number of salbutamol tablets taken in the lagundi group was 27. Of the 4 patients in the theophylline group, 1 patient took 3 tablets and 3 patients took 1 tablet each. Total number of salbutamol tablets taken in the theophylline group was only 6. No statistical analysis was employed to analyze the difference between the 2 treatment groups in terms of the number of additional medications taken but it seems apparent that theophylline patients fared better than the lagundi patients in that they took less salbutamol tablets.
Two (2) patients in the lagundi group complained of vomiting; another 2 noted desquamation of the skin over their palms and another complained increase frequency (but not amount) in urination. Three (3) patients in the theophylline group complained of nausea and one of them vomited; 2 complained of cold sweats and palpitations; another 2 complained of headaches; 1 complained of epigastric pain and another one complained of dizziness. CONCLUSION AND RECOMMENDATIONS Results of this study showed lagundi caused significant bronchodilating activity and had fewer side effects. Although theophylline has a slight edge in terms of therapeutic efficacy, yet lagundi still holds to be a promising drug in the future. The lagundi tablets used were but made from crude dried leaves and might contain only minimal active compounds. Thus, the dosage used although at 15 mg/kg/dose might actually be inadequate. Further investigations must be undertaken and the following steps are recommended: 1. Active principal should
be isolated The increasing uses of medicinal plants, the present return to Mother Earth and nature’s product, the number of people from all over the world who rely partly or completely on herbal cures and the success they achieve, are clear indications of the position these plants occupy in the practice of medicine today. In our country, the cost of imported medicine is becoming prohibitive. This shows us clearly the urgent need for extensive research on our medicinal plants. Never before had we been so forced to rely upon our own resources as we are then when the very life of our nation (for people are the nation) depend upon the herbs that God had graciously given us. LAGUNDI IS A SPARK AND
WE HOPE APPENDIX A Grading of Asthma Grade 1 A Patient only able to carry out housework or job with great difficulty. Sleep infrequently disturbed. Grade 1 B Patient only able to carry out housework or job with great difficulty. Sleep frequently disturbed. Grade 2 A Patient confined to the chair or bed but able to get up with great difficulty. Sleep is disturbed with little or no relief from inhaler. Grade 2 B Patient confined to chair and bed and only able to get up with great difficulty. Unable to sleep. Pulse rate over 120/min. Grade 3 Patient totally confined to chair or bed. No sleep. No relief from inhaler. Pulse rate over 120/min. Grade 4 patient immobilized and totally exhausted. ACKNOWLEDGEMENT The author is indebted to the following persons and institutions for their invaluable advise and assistance in making this research possible: Nelia Cortes-Maramba,
M.D. Dina de Leon, M.D. REFERENCES
Fishman, A. Pulmonary Diseases and Disorders. MacGraw Hill Book Co. c. 1980. pp. 560-576; 582-592 Goodman, L., Gilman, A. The Pharmacologic Basis of Therapeutics Sixth Edition. MacMillan Co. c. 1985. pp 358-369 Ladion, H. Healing
Wonders of Herbs. Philippine Publishing House. C.1985. pp. 14, 18, 25, 32-33,
104 Quisumbing, E. Medicinal
Plants of the Reins Atschul, S. Drugs and Foods from Little-Known Plants.
Figure 1. MEAN PEFR
VALUES OF LAGUNDI AND THEOPHYLLINE
Figure 2 MEAN PULSE RATE OF LAGUNDI AND THEOPHYLLINE
|

|

|
|
Copyright © 2002 Altermed Corporation. All rights reserved.