
Homepage maintained by C. Savona-Ventura
| Home |
| Maltese
Epidemiological Information |
| Maltese
Medical History |
| Maltese Medical Links |
A historical perspective in a central Mediterranean Island Community
Introduction
Many important
discoveries have been made in the last five decades in the field of
hereditary
mechanisms, environmental teratogenesis, prenatal diagnosis and
medical/surgical
management of affected individuals with congenital malformations.
The Maltese group of islands occupies a central position in the Mediterranean, being only 93 km away from Sicily and 290 km from Northern Africa. This location made the Islands an important meeting place for the various Mediterranean cultures throughout the ages. The history of malformations in the Maltese Islands reflects the cultural links with the mainland Mediterranean. The attitude towards congenital malformations can be divided into two periods - the Period of Superstitious belief which reflected primitive man's concepts and prevailed to at least the 17th century; and the Period of Modern Thought which began during the 18th century but made the most progress during the twentieth century.
The Period
of Superstitious Belief
Congenital
malformations causing deformities have been described since early
times.
Primitive man's interest in these phenomena has found expression in
drawings,
carvings and sculptures throughout the world including Australia, the
South
Pacific Islands, and the Americas. Written records of congenital
malformations
have come down from Babylon in the form of clay tablets from the Royal
Library of Nineveh which was assembled by the Assyrian King
Asshurbanipal
(c.700 BC). These tablets include a list of sixty-two human
malformations
with their associated prophetic implications [1,2]. It is
believed that these records date back to 4000 BC. Direct evidence of
congenital
malformations in primitive cultures were found in skeletal remains of
affected
individuals, such as a specimen of an open sacrum and a femur described
from Neolithic France with changes suggestive of congenital dislocation
of the hip [3]. The first treatise on monsters appeared in the
sixth century AD by Isidore of Seville who described numerous
abnormalities
and tried to give natural reasons for their occurrence, although
supernatural
causes were not discounted. From the mid-16th to the mid-17th
centuries,
several books on monstrous births were published and a number of
authors
published a variety of collections of such births and discussions on
their
cause [4].
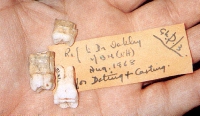
| The Maltese skeletal archaeological record shows evidence of congenital abnormalities which date to the Palaeolithic era, circa 18,000 years ago. Two teeth with taurodontism (figure 1) were found in association with remains of Cervus (deer) [5]. Taurodontism was a common feature in Homo neanderthalis, but in a minor form is also found in modern man, particularly in association with genetic anomalies such as the presence of an extra X or chromosome 21 and Prader Willi syndrome. Neolithic skeletal remains excavated from Brochtorff Circle at Xaghra (Gozo) have identified other congenital skeletal malformations and non pathological anomalies. |
 |
| These malformations include a case of a sacral spina bifida in Tarxien Phase material. Other abnormalities include absence of the sagittal suture (figure 2) in a skull from Hal Saflieni Hypogeum (Malta) [6]. |
 |
| The earliest depicted congenital malformations in Malta date from the Neolithic era and include cases of abnormalities of the hand: one with three digits and one with six digits (figure 3). These representations were discovered in an incised decoration from Gzibbu Tombs at Zebbug (Malta) and a statuette from Hagar Qim. Polydactyly is also evident in a hand print described from the Hal Saflieni Hypogeum [6-8]. |
 |
Other skeletal remains showing congenital anomalies were excavated from Roman tombs. This included a non-pathological anatomical variation of the sacrum. Here the transverse process of the first sacral vertebra was not fused with the rest of the bone. In addition two adult skulls from St. Agatha Catacombs showed features of non-union of the frontal bones [9,10]. The archaeological skeletal record also describes a number of late medieval/early modern congenital anomalies from excavations of burials in Maltese churches. These skeletal anomalies included diverse sacral anomalies including a case of spina bifida and other minor anatomical variations [11,12].
The written records of the hospitallier period furnish a number of descriptions of congenital malformations which appeared before the Episcopal court, the Inquisitional Tribunal or the Civil Courts. The first congenital malformation described in Malta dates to 1542, a case of severe male genital malformation (hypospadias) which appeared before the Episcopal Court as a case for marriage annulment. Another case of severe hypospadias was described in 1744 in the Law courts for the legal change of sex registration [13,14]. In 1630 a description of an abnormal infant was submitted by the midwife Oliveria Gambino to the Episcopal Court to justify why a stillborn was not buried in consecrated ground. The description suggests that the parturient mother gave birth to two macerated monsters - one with human and the other with avian features [15].
The theory of supernatural causes for the development of congenital malformations held sway from prehistoric time well into the seventeenth century. Congenital malformations in the various cultures and religions were often regarded as a punishment from the gods. With the advent of Christianity to the Islands, fetal anomalies were believed to originate along biblical beliefs by copulation between a woman and a male beast or between a woman and the devil. The birth and death of a grossly malformed infant or monster posed an intriguing quandary to the canonists. The officiating priest was enjoined to examine the monster to ascertain that its principal parts, namely the head and chest, had a human configuration. If they did, the infant was baptised, but if the head was that of an animal and the limbs those of a human, the creature was baptised sub conditione si es homo ego te baptizo. As late as the mid-nineteenth century canonists were still debating the religious issues raised by the birth of monsters. In their conclusions they were swayed by the conviction that these deformed beings were the result of copulation between a woman and a male beast or devil [16]. The belief was prevalent in 17th century Malta that consort with the devil in an assumed form was possible. In 1647, 17-year old Gertrude Navarre accused herself before the Inquisitional Tribunal of having over the previous six years had carnal relations with men and animals brought to her by the devil. She became pregnant and procured abortion on several occasionsn [17]. In 1676, a Maltese physician's wife accused herself of having invoked the devil and invited him to have sexual relations with her if he destroyed her husband [14].
Another aetiological theory was that of maternal impressions i.e. states of mind, affecting fetal development. However, John Hunter presented scientific evidence against maternal impressions in the late 18th century [4]. In Malta maternal impressions were also considered important aetiological factors. In the 1749, the Maltese physician Dr. Salvatore Bernard adhered to the theory that the fantasy organ of the pregnant woman communicated by means of animal spirits with the fantasy organ of the foetus, so that any perception aroused in the mother's mind produced a similar impression in the fetal brain, which impression in turn reacted upon and moulded the form of its body. Dr. Bernard held that monsters having the shape of animals and devils were born to women who, during pregnancy, had been exposed to the sight of these creatures [18,19]. These beliefs remained ingrained in Maltese mentality until relatively recent times, and many congenitally malformed individuals were kept hidden away from view by their families. A special hazard of pregnancy was the emergence of longings or desires which could not be satisfied. According to popular belief, the new-born will manifest a birth-mark resembling in form and colour the object of the unfulfilled desire. If a person neglects to satisfy the wishes of a pregnant woman, he/she would be punished by suffering from a stye [20,21]. This view was not universal. In 1804, Dr. Francisco Butigiec did not share the notion that "in an alteration of imagination which affected the foetus in such a way as to produce a defective baby or a monstrosity" [22,23].
The Period
of Modern Thought
Modern
Science was born in the 15th and 16th centuries during
the Italian Renaissance. The Renaissance initiated a process, which
during
the eighteenth century, saw the beginnings of modern attitudes towards
the aetiology of malformations. The developmental arrest theory of
teratogenesis
was first developed by William Harvey (1651) who reasoned that cleft
lip
in human infants was very similar to the normal situation found in
early
embryos. This concept was extended to explain ectopia cordis and
gastroschisis.
Although not totally understood, inherited anomalies had been
recognised
by Ambroise Pare (1649) and John Hunter (1775). However the genetic
theory
as a cause of malformations gained momentum when the inheritance laws
described
by Gregor Johann Mendel (1865) were rediscovered in 1900 by Carl
Correns,
Hugo de Vries, and Erich von Tschermak [24].
| In Malta, superstitious concepts regarding the aetiology of congenital malformations apparently persisted well into the eighteenth century, though an academic interest in the condition was being taken by medical practitioners. A case of severe malformation was described in 1788 by Dr Saverio Fenech (figure 4). The report records the birth of a monster born to a woman at Nadur. The child had a head and ears which resembled those of a cat. The upper limbs were human-like but without articulations, the hands being similar to those of a cat. The genital parts were also similar to those of a female cat. The attention given to the description, together with the added comment that the attending priest considered these characters as conforming more to a human form requiring Christian burial suggests that the religious concepts regarding malformations were still prevalent. This was not surprising since these concepts remained prevalent until the early decades of the twentieth century [14]. |
 |
Medical publications in Malta during the nineteenth century do not shed light on the beliefs prevalent among Maltese practitioners regarding the aetiology of congenital malformations. However, the description of a Maltese family in 1891 with a genetic predisposition to having twenty-four digits suggests that the hereditary theory was being entertained for at least some anomalies [25].
Other cases of malformation were described for academic purposes by medical practitioners during the nineteenth century. A case describing the internal and external features of conjoined twins with one head was described in 1816 [26], while further cases of malformed babies born in Malta were published in the 1840s [27-29]. A case of obstructed labour resulting from fetal malformation causing gross enlargement of the liver was described in 1891. The infant also had a cervical spina bifida and extra digits [25]. Prof. Giuseppi Schembri in 1896 referred to malformations which may occur, including conjoined twinning with head fusion and union by the chests, or by the pelvis giving rise to two complete trunks with two or four legs. He also listed a number of malformations that could be met by midwives, including atresia of the rectum, ears, and urethra; hypospadias; harelip and cleft palate; congenital protrusion of bowels within the naval string; conjoined or supernumerary fingers or toes; club foot; spina bifida situated at the neck and the lumbar region; hydrocele; port-wine stains, mother's marks, moles, and tongue tie [30].
| There is evidence of a three-legged conjoined twin who lived in Malta for some time in the early twentieth century. Photographs taken in Malta of a seven to nine year old child with this anomaly have been found among the belongings of Professor Ruggiero Busuttil (figure 5). The origins of this child remain unknown, and it has been suggested that the child may have been the same three-legged Francisco Lentini who was born in Sicily in 1889 and who later emigrated to America where he joined a number of circuses31. |
 |
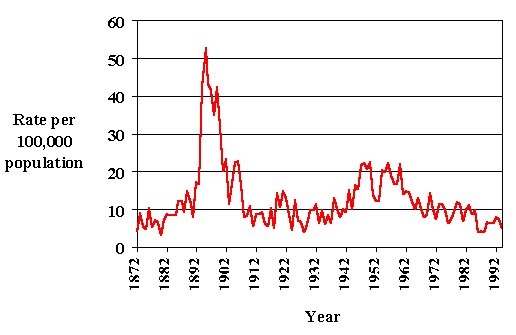
Further to the list given by Prof. Schembri in his lecture notes to midwives in 1896, there is to date no further identifiable historical material which deals with the epidemiology of abnormalities. Published mortality data suggests that in 1896, malformations accounted for a total of 76 deaths resulting in a specific mortality rate of about 43.1 per 100,000 population. All of these deaths occurred in children under five years of age. The number of deaths from malformations apparently decreased in the first decade of the twentieth century to eventually maintain an annual fluctuation around 8.5 per 100,000 population in the 1920s. The specific mortality rate from congenital malformations started to rise just prior to the Second World War to peak to a value of about 18 per 100,000 population in the 1950s. After the 1950s, the specific mortality rate fell progressively to reach mean values of about 7 per 100,000 population in the 1980s. The majority of these deaths occurred in childhood so that the annual childhood mortality rate from congenital malformations during 1981-85 was 54.2 per 10,000 total births. The larger proportion of these deaths throughout the years was caused by congenital heart lesions, with the second commoner group of malformations being abnormalities of the central nervous system including hydrocephalus and spina bifida [32-35] (figure 6).
 |
|
|
While a number of studies had been undertaken by individual clinicians in Malta on specific congenital disorders36-39, epidemiological study of congenital malformations in Malta was seriously initiated in the early 1980s. This lack of data is not surprising in view of the fact that before the First International Conference on Congenital Malformations in 1960, there were very few studies in the world literature on incidence of congenital malformations [40,41].
A small preliminary survey of congenital anomalies in live-born Maltese children was performed in 1972 reporting 20 anomalies in a total of 1016 consecutive births [42]. In 1983, a computerised database was initiated by the Department of Obstetrics and Gynaecology in order to allow the registration of all births at Karen Grech Hospital. This database allowed a number of epidemiological studies to be initiated. Malformations were shown during 1983-1886 to occur in about 3.5% of all births, with minor malformations accounting for about 77% of all malformations. While minor malformations were shown to be approximately the same in all age groups, the major malformation rate increased with increasing maternal age [43]. A further database was initiated after 1986 by the Departments of Genetics and Obstetrics-Gynaecology in conjunction with the EUROCAT Project. This project is a concerted action of the European Union in the epidemiology of congenital anomalies. The EUROCAT data base initiated in 1978 has indicates that the malformation rates in Europe should range from a minimum of 0.9% to a maximum of 4.6%. The EUROCAT project has further shown that the incidence of anomalies caused by chromosomal problems in Europe varied in incidence from 9.4 - 22.3 per 10,000 total births. Of all the registered cases, approximately 74% were Down Syndrome [44]. In Malta during the period 1983-87, the prevalence of chromosomal abnormalities was estimated at 22.0 per 10,000 births or a frequency at 1:434. The prevalence of Down Syndrome in Malta was estimated at 18.8 per 10,000 births (frequency 1:532) or 85.5% of chromosomal anomalies diagnosed. The frequency of Down Syndrome was markedly higher in older mothers. The lowest risk of occurrence appears to be in the 25-34 year age group, and it is approximately three times higher in mothers below 20 years and 25-30 times higher in the 40-45 years age group [45-47].
The last decade has seen further efforts at epidemiological studies with the continuation of the EUROCAT Project and the establishment of the Malta Congenital Anomalies Register, and the initiation of several databases to assess the incidence and prevalence of specific congenital malformations particularly thalassaemia (Laboratory of Molecular Genetics) and congenital heart disease (Maltese Paediatric Cardiology Database).
CONCLUSION
Though magico-religious and superstitious concepts no longer come to the fore, the twentieth century concepts towards congenital malformations are not very different from the past. There is at present little that can be done further than pre-pregnancy counselling and pre-natal diagnosis/abortion to decrease the incidence of congenital abnormalities. Advances have been made over the last decades in the medical and surgical management of individuals to enable them to overcome physical handicaps and live a health life. Problems with regards to assimilation of the individual with a physical, and more so mental, handicap still remain in the social field. Over the last fifty years, it appears that the medical and social community changed the terminology regarding mental retardation earning a few new syllables every few decades. Labels have varied from "moron" to "feebleminded", to "mental defective", then to "mentally retarded" and finally "developmentally disabled". In Malta this phenomenon has been noted at a faster pace in the last decade or so, with labels changing from "immankati" [deformed], to "handikappati" [handicapped], then to "persuni b'disabilita`" [persons with disability] and finally "persuni bzonnijiet specjali" [people with special needs]. One hopes that the change in terminology will have more tangible long-term effects on the outlook towards these individuals and the services offered to address their needs. In 1992 the American Association on Mental introduced "a revolutionary new way of defining mental retardation". People are never mentally retarded in an absolute sense: rather they have different "intensities of functional needs". Communities, by structuring themselves to meet those functional needs, can "cure" mental retardation. In other words, a person ceases to be mentally retarded the moment people quit defining him as such. That hopeful philosophy found its fictional apotheosis in the film Forest Gump. Born with an IQ that types him as mentally retarded, Gump changes the course of American history because his mother refuses to acknowledge his limitations. He is admitted to a regular public school, reaches college on a football scholarship, and becomes a war hero, ping-pong champion, millionaire and spiritual leader. However many who cheer Gump's story are less willing to indulge his real-world counterparts. The question still remains whether a simple redefinition can change attitudes towards mental retardation, or whether a fate worse than labelling still awaits those at the bottom of the statistical curve?.
References
- Brodsky I. Congenital abnormalities, tetratology and embryology: Some evidence of primitive man's knowledge as expressed in art and lore in Oceania. Med J Australia 1943;1:417
- Warkany J. Congenital malformations in the past. J Chron Dis 1959;10:84-96
- Sigerist HE. A History of Medicine. 1: Primitive and Archaic Medicine. New York;Oxford University Press, 1967: 45-50,54,57-58
- Barrow MV. A brief history of teratology to the early twentieth century. Teratology 1971;4:119-130
- Mifsud A, Mifsud S. Dossier Malta. Evidence for the Magdalenian. Malta;Proprint, 1997
- Savona-Ventura C, Mifsud A. Prehistoric Medicine in Malta. Malta;Proprint, 1999
- Pace JL. The Anatomical features of Prehistoric Man in Malta. Malta;The University of Malta, 1972:14
- Zammit T, Singer C. Neolithic representation of the human form from the Islands of Malta and Gozo. J Roy Anthropol Inst 1924, LIV:81
- Cassar P. Medical History of Malta. London;Wellcome Hist Med Libr, 1964: 8-9
- Savona-Ventura C, Mifsud A, Camilleri V. The Anthropomorphology of Classical Skulls from Malta-in press
- Pace JL, Ramaswamy S. The Finds: Skeletal remains. In: Blagg TFC, Bonanno A, Lutrell AT, ed. Excavations at Hal Millieri, Malta: a report of the 1977 campaign conducted on behalf of the National Museum of Malta and the University of Malta. Malta;University Press, 1990;84-95
- Ramaswamy S, Pace JL. The Medieval skeletal remains from St. Gregory’s Church at Zejtun (Malta). Part 1. Paleopathological Studies. Arch Ital Anat Embriol 1979;LXXXIV(1):43-53
- Cassar P. A medico-legal report of the sixteenth century from Malta. Medical History 1974;18:354-359
- Cassar P. Change of sex sanctioned by a Maltese law court in the eighteenth century. BMJ 1954;2:1413
- Cassar P. The birth of monsters in the Maltese Islands in the 17th and 18th century. Mediscope 1983;1:6-9
- Savona-Ventura C. The influence of the Roman Catholic Church on Midwifery Practice in Malta. Medical History 1995;39:25-26
- Bonnici A Maltin u l-Inkizzjoni f’nofs is-seklu sbatax. Malta;Klabb Kotba Maltin, 1977;102-104,199-200
- Bernard S. Trattato filosofico-medico dell'uomo. Catania, 1749
- Cassar P. The Neuro-psychological concepts of Dr. S. Bernard. Scientia 1949;15:29
- Cassar Pullicino J. Studies in Maltese Folklore. Malta;University Press, 1992;213-215
- Cassar P. Pregnancy and birth in Maltese tradition. Chestpiece 1975:25
- Bardon S. Trattato Dell'Arte Ostetrica dettato e spiegato dal Perille Signo Dr. Francesco Butigiec nello Studio Publico del Grand'Ospedale Nazionale de' Maltesi. Principiato li 18 ottobre 1804. Manuscript lecture notes, +247fols.
- Cassar P Teaching of Midwifery in Malta at the beginning of the 19th century. St. Luke's Hosp Gaz 1973;8:91-111
- Sturtevant AH. A history of genetics. New York;Harper & Row, 1965;9-32
- Gulia G. Di un caso di distocia per volume esagerato del fegato fetale - Monstruosita` ed anomalia del bambino. La Rivista Medica, 30 September 1891, Anno II(14):8
- Anon. An account of a monstrous fetus born in Malta in 1816. No place or date of publication. C.1816
- Anon. Il Portafoglio Maltese, 13 April 1840, p.851
- Anon. Il Portafoglio Maltese , 5 June 1843, p.2247
- Anon. Storia della societa’ medica d’incorraggiamento di Malta. 1845;xxxiv,6,52,255
- Schembri GB The Midwife's Guide Book. Malta;Government printing Office, 1896, 76
- Mizzi C Il-misteru dwar it-tifel bi tliet saqajn. It-Torca, 15 April 1990, 14-15;22 April 1990, 14-15,24
- P.H.D.: Return of Deaths in Malta and Gozo. Malta Government Gazette, 1872-1896 [fortnightly reports published by the Public Health Department]
- D.O.H. Annual Reports on the Health Conditions of the Maltese Islands and on the work of the Medical and Health Department for the years 1896-1970. [annual publications published as supplements of the Malta Government Gazette or as Departmental publications], 1897-1971
- C.O.S. . Demographic Review of the Maltese Islands 1960-1994. Malta;Central Office of Statistics [annual publications], 1961-1996
- Savona-Ventura C, Grech V. Congenital malformations in a central Mediterranean island. Int J Risk Safety Med 1997;10:31-39
- Cachia EA, Fenech F. Incidence of congenital pyloris stenosis in Malta. J Med Genet 1966;3:49
- Cassar P. Huntington's Chorea, with special reference to its incidence in Malta. St. Luke's Hospital Gazette 1967;2:3-13
- Cauchi MN. Glucose-6-Phasphate Deficiency in Malta - A Preliminary Study. St. Luke's Hospital Gazette 1968;3:30-33
- Vella F. The frequency of Thalassaemia minor in the Maltese Islands. Acta Haematologica 1962;27:278
- Kennedy WP: Epidemiologic aspects of the problem of congenital malformations. Birth Defects Orig. Artic. Ser. 1967;3:1-18
- Lamy M, Frezal J. The frequency of congenital malformations. First International Conference on Congenital Malformations. Philadelphia;Lippincott 1960: 34-44
- Jaccarini CJ, Vassallo-Agius P. Congenital malformations survey. A preliminary report. St. Luke's Hospital Gazette 1972;7:25-29
- Grech ES, Savona-Ventura C, eds. Proceedings: European Study Group on Social Aspects of human Reproduction. V Annual meeting, Malta, September 1987. Malta;Government Press, n.d., [1988]
- Wals De, P;Dolk H, Weatherall JAC, et al. Prevalence of congenital anomalies in 19 EUROCAT countries, 1979-1982. In: De Wals P, Weatherall JAC, Lechat MF, eds. Registration of congenital anomalies in EUROCAT Centres 1979-1983. Belgium;Cabay, 1985: 146-202
- Cuschieri A, 1987: Registration of congenital anomalies in Malta. In: De Wals P, Lechat MF, eds. EURCAT Report 2: surveillance of congenital anomalies years 1980-1984. Belgium;Catholic University of Leuven, 1987: 243-248
- Cuschieri A, Gauci S. A Survey of Chromosomal Anomalies in Malta. Maltese Medical Journal 1988;1:38-43
- Cuschieri A, 1993: A survey of Congenital Anomalies in Malta. In: R. Ellul-Micallef, S. Fiorini, eds. Collected Papers published on the occasion of the Collegium Melitense Quatercentenary Celebrations (1592-1992). Malta: University of Malta, 1993: 221-244

It would be appreciated if source acknowledgement is made whenever any material is used from this source.
Citation: C. Savona-Ventura: The Health of the Maltese Population. Internet Home Page [http://www.oocities.org/savona.geo/index.html], 1996