-
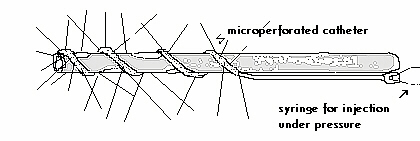
Figure 1
 Original Article
Original Article
We developed a "Thoracic drain with a coupled microperforated injector catheter"
(PLEURODREN) to diminish the intensity of post-drainage pain
.(Figure 1).
PATIENTS AND METHODS
We utilized the PLEURODREN in 54 patients: 24 toracothomies and in 30 pleural drainages. Analgesia was obtained through injection under pressure of fractioned doses of lidocaine (2% xylocaíne, 4 ml every 6 hours) thus sprinkling the anesthetic in the pleural surface.
In the immediate post-operatory period and until the removal of the thoracic drain(s) respiratory function was evaluated in 12 patients, before and after the injection of the anesthetic through the PLEURODREN as a measure to evaluate and gauge functional improvement correlated with decreased pain. The items studied were: Vital Capacity (VC), Forced Expiratory Volume 1s (FEV1) , Maximal Inspiratory Pressure (PiMx) and Maximal Expiratory Pressure (PeMx)
Subjective pain intensity was evaluated according to the analogue scale of Huskisson (1)
RESULTS
In the post-operatory period we observed, for each patient, an improvement of 80% in the intensity of pain following analgesia. Improvement was referred very soon after injection of the anesthetic by the majority of patients and correlated positively with improvement in respiratory function (Table 1).
TABLE 1 - RESPIRATORY FUNCTION FOLLOWING ANALGESIA.
| % INCREASE* | |
|---|---|
| VC | |
| FEV1 | |
| Pi máx | |
| Pe máx |
COMMENTS
Analgesia is a key element for a well succeeded convalescence following a thoracic surgery. Postoperatory pain is originated from the surgical trauma to the tissues as well as from inflamatory response. Different alternatives are used to treat postoperatory pain. These include(2): the use of narcotics, intercostal blocks, epidural analgesia and the use of anti-inflamatories.
The results with the use of PLEURODREN , accentuated decrease in the intensity of postoperatory pain, qualify its use as an adequate alternative in the treatment of pain following a thoracic procedure.
REFERENCES
(1)Huskisson EC. Measurement of pain. Lancet 1974;1:1127
(2)Kavanagh BP, Katz J, Sandler AN. Pain control after thoracic surgery. A review of current techniques. Aanesthesiology 1994;81:737

