Advanced Life Support
-
2005 AHA Guidelines for Emergency Cardiovascular Care
Advanced Cardiac Life Support (ACLS)

Pediatric Advanced Life Support (PALS)



Advanced Trauma Life Support (ATLS)
-
Primary Survey:
The most immediately lethal injuries are taken care of as they are identified.
-
Airway
Clear airway: chin lift, suction, finger sweep
Protect airway
Breathing
Ventilate with 100% oxygen
Check thorax and neck
Deviated trachea
Tension pneumothorax (intervention: needle decompression)
Chest wounds and chest wall motion
Sucking chest wound (intervention: occlusive dressing)
Neck and chest crepitation
Multiple broken ribs
Fractured sternum
Pneumothorax
Listen for breath sounds
Correct tracheal tube placement?
Hemopneumothorax?
Chest tube(s) ≥38-Fr
Collect blood for autotransfusion
Circulation
Apply pressure to sites of external exsanguination
Assure that two large-bore IVs established
Begin with rapid infusion of warm crystalloid solution
If arm sites unavailable, insert a large central line or perform a saphenous cutdown at the ankle
Assess blood volume status
Radial and carotid pulses
BP
Jugular venous filling
Quality of heart tones
Beck triad (↓ BP, ↑ CVP, distant heart sounds)?
Hypovolemia
After 2 L of crystalloid begin blood infusion if still hypovolemic; in children use two 20-mL/kg boluses then 10-mL/kg blood boluses if still unstable
Near-term pregnant patient: place roll under right hip
Disability
Brief neurologic examination
Pupil size and reactivity
Limb movement
Glasgow Coma Scale
Exposure
Completely disrobe the patient
Logroll to inspect back
Monitor fluid administration
Consider central line for CVP monitoring
Use fetal heart rate as indicator in pregnant women
Secondary Survey:
A thorough search for injuries is carried out in order to set further priorities.
- Trauma series x-rays: lateral cervical spine, supine chest, AP pelvis
Head-to-toe examination looking and feeling; quickly bring problems under control as they are discovered
Scalp wound bleeding controlled with Raney clips
Hemotympanum?
Facial stability?
Epistaxis tamponaded with balloons if severe
Avulsed teeth, broken jaw?
Penetrating injuries?
Abdominal distention and tenderness?
Pelvic stability?
Perineal laceration/hematoma?
Urethral meatus blood?
Rectal examination for tone, blood, and prostate position
Bimanual vaginal examination
Peripheral pulses
Deformities, open fractures
Reflexes, sensation
Large gastric tube ≥18-Fr inserted
Foley catheter inserted
Blood?
Pregnancy test
Logroll the patient to feel and see the back, flanks, and buttocks if not already done
Splint unstable fractures/dislocations
Assure that tetanus prophylaxis is given
Consult with surgeon regarding further tests or immediate need for surgery or preferred IV medications; consider:
-
Emergency thoracotomy to provide aortic compression or cross-clamping
rule out ruptured aorta → aortogram or upright chest x-ray to
pelvic fracture or hematuria → cystogram, IVP, or enhanced abdomen CT
FAST (focused assessment with sonography for trauma) or DPL (diagnostic peritoneal lavage)
Head CT
neurologic decompensation → IV mannitol for
possible spinal cord injury → IV steroids
possible ruptured abdominal viscus → IV antibiotics
perineal, vaginal, or rectal lacerations → IV antibiotics
pelvic hemorrhage → pelvic arteriogram and embolization

Apgar Scoring System
Sign |
0 Points |
1 Point |
2 Points |
Heart rate |
Absent |
<100 |
>100 |
Respiratory effort |
Absent |
Slow, irregular |
Good, crying |
Muscle tone |
Flaccid |
Some flexion of extremities |
Active motion |
Reflex irritability |
No response |
Grimace |
Vigorous cry |
Color |
Blue, pale |
Body pink, extremities blue |
Completely pink |
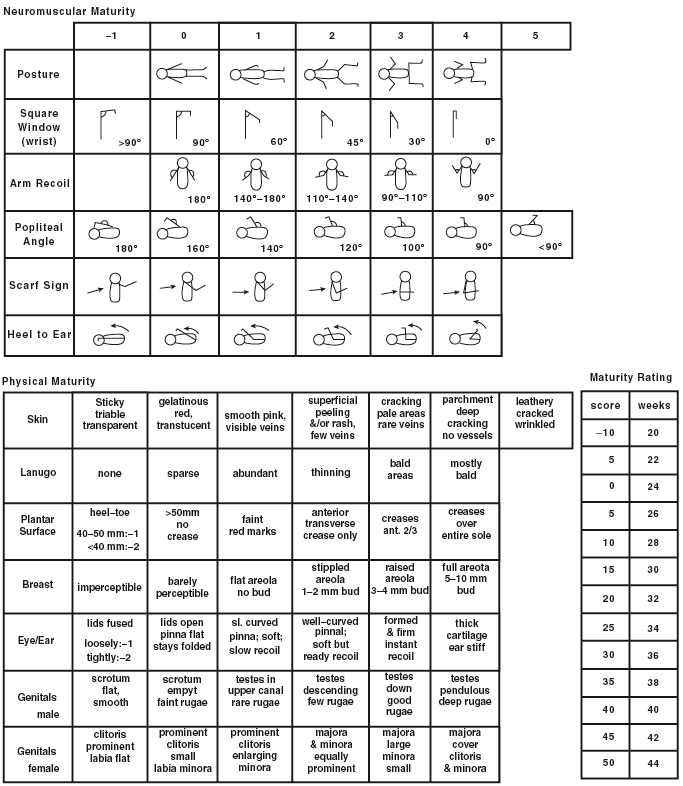
Ballard score for estimating gestational age
Stroke

| Table 3: Use of tPA in Patients With Acute Ischemic Stroke (All boxes must be checked before tPA can be given.) |
| Inclusion Criteria(all Yes boxes in this section must be checked): |
| Yes |
| ∅ Age ≥ 18 y/o? |
| ∅ Clinical diagnosis of ischemic stroke with a measurable neurologic deficit? |
| ∅ Time of symptom onset (when patient was last seen normal) well established as <180 minutes (3 hours) before treatment would begin? |
| Exclusion Criteria (all No boxes in "Contraindications" section must be checked): |
| Contraindications: |
| No |
| ∅ Evidence of intracranial hemorrhage on pretreatment noncontrast head CT? |
| ∅ Clinical presentation suggestive of subarachnoid hemorrhage even with normal CT? |
| ∅ CT shows multilobar infarction (hypodensity greater than one third cerebral hemisphere)? |
| ∅ History of intracranial hemorrhage? |
| ∅ Uncontrolled hypertension: At the time treatment should begin, sBP >185 or dBP >110? |
| ∅ Known arteriovenous malformation, neoplasm, or aneurysm? |
| ∅ Witnessed seizure at stroke onset? |
| ∅ Active internal bleeding or acute trauma (fracture)? |
| ∅ Acute bleeding diathesis, including but not limited to:
—Platelet count <100 000/mm3? —Heparin received within 48 hours, resulting in aPTT > upper limit of normal? —Current use of anticoagulant (eg, warfarin) that has produced an elevated INR >1.7?* |
| ∅ Within 3 months of intracranial or intraspinal surgery, serious head trauma, or previous stroke? |
| ∅ Arterial puncture at a noncompressible site within past 7 days? |
| Relative Contraindications/Precautions: |
| • Only minor or rapidly improving stroke symptoms (clearing spontaneously) |
| • Within 14 days of major surgery or serious trauma |
| • Recent gastrointestinal or urinary tract hemorrhage (within previous 21 days) |
| • Recent acute myocardial infarction (within previous 3 months) |
| • Postmyocardial infarction pericarditis |
| • Plasma glucose <2.8 or >22.2 mmol/L |
-
*In patients without recent use of anticoagulants, treatment with tPA can be initiated before availability of coagulation study results but should be discontinued if the INR >1.7 or ↑ PTT.
Brief neurological exam
-
Level of Consciousness
-
Alert: normal consciousness
Drowsy: wakens when stimulated verbally but tends to doze off to sleep
Stuporous: responds to loud stimuli but does not become alert (→ GCS)
Comatose: responds to deep pain only (→ GCS)
Pupils
Orientation
-
time, place, person
Speech
-
Normal: can be slurred but intelligible.
Expressive dysphasia: Ask the patient to name 3 objects, e.g. pencil, key, and watch. Then ask “what do you do with a key?...a watch?...and a pencil?
Receptive dysphasia: Ask patient to follow three commands: Close your eyes, point to the ceiling, and wiggle toes. (Do not mimic commands.)
Motor
-
Face: symmetry
Arm:
- Proximal
Distal
- Proximal
Distal