Nuclear Medicine Gamuts
Leonardo
Double-click → opens on left screen
Shift & double-click → opens on right screen
![]()
![]()
Brain
Tc-99m pertechnetate-HMPAO, Tc-99m ECD, N-13-ammonia (PET) are perfusion agents, lipophilic & extracted on first pass.
Diamox → vasodilation of Nl areas → worsened perfusion in areas of vascular dz.
Tl-201, F-18-FDG (PET) are metabolic agents with activity in tumors but not in areas of radiation necrosis.
Indium-111-DTPA intrathecally for CSF leak or NPH.
| Multiple, asymmetric cortical perfusion defects | Multi-infarct dementia, vasculitis, coccaine abuse |
| Symmetrical ↓ activity in posterior parietal-temporal lobes; preserved activity in calcarine cortex & basal ganglia | Alzheimer's dz (not specific) |
| ↑ activity temporal lobe | Herpes encephalitis |
| ↑ perfusion & ↑ metabolism during seizure; ↓ or Nl activity interictally | Seizure focus |
| Lack of intrathecally-administered Indium-111-DTPA activity superior surface of brain after 1-2 days | Indicates NPH |
![]()
Thyroid
| Tc-99m pertechnetate | IV | trapped |
| Radio-iodine, e.g. I-123 | PO | trapped & organified |
Discordant nodule: Some Ca are hot using Tc-99m pertechnetate & cold using I-123.
Thyrotoxicosis
| Condition | %RAIU | Scan | |
| Grave's dz | ↑ | Enlarged, homogeneous | |
| Toxic multinodular goitre (Plummer's dz) | hi Nl or ↑ | Hyperfunctioning nodules, suppressed extra-nodular tissue | |
| Hashitoxicosis (rare, transient) (chronic thyroiditis) (lymphocytic infiltn) | ↑ | Enlarged, patchy | |
| Toxic nodule (adenoma) | usu. Nl | Hyperfunctioning nodule, suppressed extra-nodular tissue | |
| Subacute thyroiditis E.g. de Quervain's (granulomatous) thyroiditis, silent thyroiditis, post-partum thyroiditis | ↓ | Nonvisualization | |
| Struma ovarii (functioning thyroid tissue in ovarian teratoma) | |||
| ↓ | |||
| ↓ | |||
| ↓ |
![]()
GI
Hepatobiliary
Tc-99m IDA (e.g. DISIDA) is excreted by hepatocytes, but not conjugated.
indicates
| Non-visualization of GB at 4 hrs or after morphine at 1 hr | likely acute cholecystitis |
| rim sign | may be gangrene, rupture, abscess |
| Non-visualization of GB at 1 hr but visualization at 4 hrs or after morphine | likely chronic cholecystitis |
| Persistent cardiac blood pool activity, poor liver activity, & no biliary excretion | hepatocellular disease (e.g. hepatitis, cirrhosis); severe biliary obstruction |
| No bowel activity by 1 hr | Common duct calculus, tumor, stricture, morphine, sphincter dyskinesia, chronic cholecystitis |
| Only liver activity & no cardiac, biliary , or bowel activity | may be "liver scan of complete biliary obstruction" |
| In neonate, no bowel activity by 24 hrs | biliary atresia, severe hepatitis |
| CCK ejection fraction | > 50% normal 35 - 50% borderline <35% abnormal - sugg acute or chronic cholecystitis |
Colloid Liver-Spleen
Tc-99m sulfur colloid
| Colloid shift: BM easily visualized; spleen activity > liver | Hepatocellular disease ( also look for ascites, hepatoma (photopenic)) |
| Photopenic lesions | Anything that not have reticuloendothelial activity (e.g. liver: cyst, hematoma, abscess, fatty infiltration, adenoma, hepatoma, mets e.g. spleen: cyst, tumor, infarct) |
| ↑ activity | FNH, regenerating nodule in cirrhosis, flow abnls |
Meckel's Diverticulum Imaging
Tc-99m pertechnetate (concentrates in gastric mucosa, in stomach or ectopic)
Pentagastrin → ↑ mucosal uptake of Tc-99m pertechnetate
Cimetidine → block release of Tc-99m pertechnetate from mucosa
Glucagon → ↓ small bowel motility
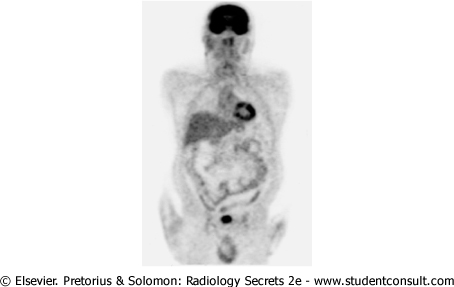
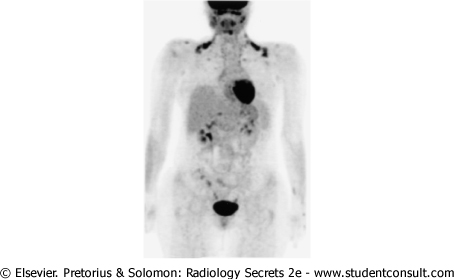
GI Bleeding Study
Tc-99m-labelled RBC's (Tc-99m sulphur colloid only if active bleeding)
![]()
GU
Kidneys
Tc-99m-DTPA: GFR
Tc-99m-DMSA: renal cortex
Tc-99m-MAG3: tubular agent
Tc-99m-glucoheptonate: renal cortex & collecting system
| Tc-99m-MAG3 → delayed clearance with signif cortical retention | Renal artery stenosis |
| Tc-99m-MAG3 → bilateral delayed clearance with signif cortical retention | Bilateral renal artery stenosis, obstruction, medical renal dz, pre-renal azotemia |
| Tc-99m-MAG3 or DTPA → delayed clearance (20 - 30 mins) with dilated intrarenal collecting system | Flaccid system or obstruction. If furosemide → rapid washout, then probab flaccid system. |
| Tc-99m-MAG3 → Nl perfusion, ↑'g cortical activity, ↑'g renograms | ATN, cyclosporin toxicity |
| Tc-99m-MAG3 → absent perfusion | Hyperacute rejection (< 24 hrs post-transplantn) |
| Tc-99m-MAG3 → poor perfusion, poor excretion | Acute rejection (2 -3 mos post-transplantn) |
Testes
| Diffusely hot | Epididymitis |
| ↓ or absent testicular flow | Torsion |
Adrenal
| NP-59 → unilateral adrenal cortical uptake | Usu adenoma |
| NP-59 → bilateral adrenal cortical uptake | Usu hyperplasia |
| MIBG → tissue localization | pheochromocytoma, neuroblastoma, paraganglioma, carcinoid, medullary thyroid Ca |
![]()
![]()
![]()
Respiratory
Modified PIOPED Criteria
| Probability | Criteria | ||
| High (> 80%) | >= 2 large mismatched segmental perfusion defects or the arithmetic equivalent | ||
| Intermediate (20% - 80%) | One moderate to < two large mismatched perfusion defects or the arithmetic equivalent Single-matched ventilation-perfusion defect with a clear chest radiograph is borderline for low probability Difficult to categorize as low or high | ||
| Low (<20%) | Nonsegmental perfusion defects (e.g.cardiomegaly, enlarged aorta, enlarged hila, elevated diaphragm) Any perfusion defect with a substantially larger chest radiographic abnormality Perfusion defects matched by ventilation abnormality provided that there are: a) clear chest radiograph; and b) some areas of normal perfusion in the lungs Stripe sign Any number of small perfusion defects with a normal chest radiograph | ||
| Very Low | <= 3 small perfusion defects ("rat bites") | ||
| Normal | No perfusion defects or perfusion exactly outlines the shape of the lung seen on the chest radiograph |
Segmental perfusion defects:
Large = >75%
Moderate = 25% - 75%
Small = <25%
![]()