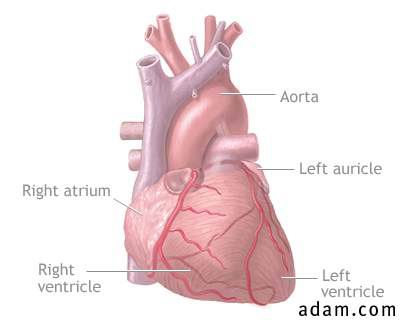
Abdominal aortic aneurysm
Aortic rupture, chest X-ray

An abnormal widening of
the abdominal portion of the aorta (the major artery from the heart).
Alternative Names
aortic aneurysm (dissecting)
A condition in which there is bleeding into and along the wall of the aorta (the major artery from the heart); this condition may also involve abnormal widening or ballooning of the aorta (aneurysm).
Causes, Incidence and Risk Factors
Aortic dissection involves
bleeding into and along the wall of the aorta (the major artery from the
heart), most often because of a tear or damage to the inner wall of the
artery. This usually occurs in the thoracic (chest) portion of the aorta but
may occur in the abdominal portion also.
The exact cause is unknown, but risks include
atherosclerosis and
hypertension. Traumatic injury is a major cause of aortic dissection,
especially blunt trauma to the chest as with the steering wheel of a car
during an accident. Aortic dissection may also be associated with other
injury, infection, congenital weakness of the aorta, collagen disorders such
as
Marfan's syndrome, pseudoxanthoma elastoma, Ehlers-Danlos syndrome,
relapsing polychondritis, or
abdominal aortic aneurysm.
Pregnancy, valve disorders (including
aortic insufficiency), and
coarctation of the aorta may also be associated with aortic dissection.
Aortic dissection occurs in approximately 2 out of 10,000 people. It can
affect anybody, but it is most often seen in men 40 to 70 years old.
-
chest pain
- sudden, severe
- sharp, stabbing, tearing, or ripping
- located below the sternum, under the shoulder blades, or in the back
- pain may radiate to shoulder, neck, arm, jaw, abdomen, hips
- location of pain may change
- changes in thought ability, concentration (confusion, disorientation)
- decreased movement, any location
- decreased sensation, any location
- anxiety
- pallor
- rapid pulse (heart rate)
- profuse sweating
- dry skin/mouth, thirst
- nausea, vomiting
- dizziness, fainting
-
shortness of breath (dyspnea)
- difficulty breathing when flat (orthopnea)
- difficulty breathing at night (paroxysmal nocturnal dyspnea)
Note: Symptoms may begin suddenly.
Additional symptoms that may be associated with this disease:
Listening with a stethoscope (auscultation)
at the chest and abdomen may reveal a "blowing" murmur over the aorta, a
heart murmur, or other abnormality. There may be decreased (weak) pulses in
the upper extremities. There may be signs of
tamponade or
hypovolemia, or signs resembling
acute
MI. There may be signs of
shock
but with normal
blood
pressure.
Aortic dissection or
aortic aneurysm may be revealed on:
- an aortic angiography
- a chest MRI or CT scan of chest
- an echocardiography
- a chest X-ray (may show mediastinal widening)
- a Doppler ultrasonography (occasionally performed)
- ECG may show signs of cardiac tamponade.
- CBC is performed to evaluate blood loss.
The goal of treatment is prevention of complications. Hospitalization
is usually required.
Antihypertensives may be prescribed to reduce
blood
pressure. These may be given through a vein (intravenous).
Analgesics may be needed for pain. Cardiac medications such as
beta-blockers may reduce some of the symptoms.
Surgical repair or replacement of the section of aorta is curative.
Aortic dissection may be life threatening. The disorder is curable with surgical repair if it is performed before aortic rupture. Less than half of the patients with ruptured aorta survive.
- bleeding from the aorta
- aortic rupture causing rapid blood loss, shock, death
- clot formation
- insufficient circulation past the area of the dissection
- irreversible kidney failure
- stroke
- myocardial infarction (tissue death)
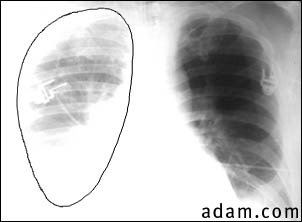
- Aortic
rupture (a tear in the aorta, which is the major artery coming from the
heart) can be seen on a chest X-ray. In this case, it was caused by a
traumatic perforation of the thoracic aorta. This is how the X-ray appears
when the chest is full of blood (right-sided hemothorax) seen here as
cloudiness on the left side of the picture.
- cardiac tamponade
Calling Your Health Care Provider
If symptoms indicate aortic dissection may be present or severe
chest pain develops, call the local emergency number (such as 911) or go
to the emergency room.
Adequate treatment and control of
atherosclerosis and
hypertension may reduce risk. Use
safety precautions to reduce the risk of injury. Many cases are not
preventable.
Infective endocarditis Aortic rupture, chest X-ray |
|
Thoracic aortic aneurysm
aneurysm - thoracic aortic; aortic aneurysm (thoracic); syphilitic aneurysm A localized dilation of the wall of the thoracic aorta caused by
atherosclerosis,
hypertension or, less commonly,
syphilis. Syphilitic
aneurysms nearly always occur at the thoracic aorta, whereas more
common aneurysms, due to atherosclerosis, nearly always occur in the
abdominal aorta. This condition is rare in children.
|