Health impact
Tuberculosis
is an infectious disease caused by a bacillus -Mycobacterium tuberculosis- that
spreads through the air when untreated TB patients cough. Left untreated, a
single person with active TB can infect 10 to 15 others each year, creating a
self-perpetuating pool of infection.
Someone
in the work! is infected with TB every second. Seven to eight million people
become sick and two million die from it each year.
Tuberculosis
has existed in India since the earliest days.
In 1500 BC, the Rig Veda described the illness as Rajayaksma,
king of diseases. Today, India accounts for nearly 30 per cent of all
tubercuiosis cases in the world, a figure that is likefy to increase as India's
population grows and the HIV epidemic progresses.
Tuberculosis
burden and control —10 countries with most cases. 1997
|
COUNTRY
|
Population
(millions)
|
Estimated
Total TB Cases
(thousands,
1997)
|
Estimated
incidence
per 100.000
per year
|
Estimated new
infectious cases
treated under
DOTS. 1997
|
New
infectious cases
|
|
India
|
960,178
|
1,799
|
187
|
805,000
|
7,708
|
|
China
|
1,243,738
|
1,402
|
113
|
630,000
|
147,905
|
|
Indonesia
|
204,323
|
583
|
285
|
262,000
|
19,492
|
|
Bangladesh
|
122,013
|
300
|
246
|
135,000
|
25.871
|
|
Pakistan
|
143,831
|
261
|
181
|
117,000
|
-
|
|
Nigeria
|
118,369
|
253
|
214
|
110,000
|
11,235
|
|
Philippines
|
70,724
|
222
|
314
|
100,000
|
3,190
|
|
South Africa
|
43,336
|
170
|
392
|
69,000
|
4,146
|
|
Russia
|
147,708
|
156
|
106
|
70,000
|
660
|
|
Ethiopia
|
60,148
|
156
|
260
|
66,000
|
15,753
|
|
Sourse: Dye C,
Scheele S,Dolin P, Pathania V ,Raviglione MC ,Global burden of
tuberculosis.JAMA ;292:677-686
|
Most adults in India have been infected with the
tuberculosis bacteria. In a 1997 review. Prevalence and incidence of
Tuberculosis infection and Disease in India, A.K. Chakraborty found that tuberculosis
is common over all of India, in both rural and urban areas. About 38 percent of
people all ages are infected with the
disease, while infection among males above
40
years of age runs as high as 70 percent.
According to the 1999 World
Health Report, the burden of tuberculosis in India is 36 times more than
leprosy, 1 3 times more than malaria, 2.5 times more than tropical diseases,
and 35% more than HIV AIDS.
More adufts
in India die fromTB than from any other infectious disease one every minute and
more than 1,000 every day - a grim statistic that has changed littte over the
past two decades.
Every year, 2
million people in India develop the disease, half of whom - more than 2,000
patients every day - have infectious and often fatal tuberculosis. Prevalence
of the disease is more than twice the incidence, indicating a failure of
current treatment programmes and a pooling up of previous cases. Unless
promptly and effectively treated, these patients will infect succeeding
generations and the cycle of infection, disease, and death from tuberculosis
will continue for centuries.
Economic impact
The burden of suffering
caused by tuberculosis in India is enormous. TB is one of India's biggest
public health problems - a problem that India can ill-afford.
Tuberculosis
and its spread remind us that we are all connected by the air we breathe.
Although
sometimes considered a disease of slums and ghettos, affecting only the
socially disadvantaged, tuberculosis can in fact affect anyone - from remote
villages to bustling urban centers. Those infected are disproportionately young
adults in the most productive years of their lives, often the primary wage
earners of their families.
ŇÂ is a disease that impoverishes families
and undermines economic development. In 1996, the World Health Organization
estimated that India loses about 400 million dollars (Rs. 1 700 crore) in
economic output every year from tuberculosis.
In
a 1997 study conducted in Tamil Nadu, researchers at the Tuberculosis Research
Centre in Chennai found that an average patient suffering from tuberculosis
incurs a total loss of Rs 3469 (US$ 99) while shopping for diagnosis and
treatment. For a daily wage laborer who might hope to earn the equivalent US$
200-400 per year, this is a prohibitive sum - equivalent to 3-6 months of
wages. This study indicates that tuberculosis may cause 300,000 children to
become orphans, and 100,000 Indian women to be rejected by their families each
year.
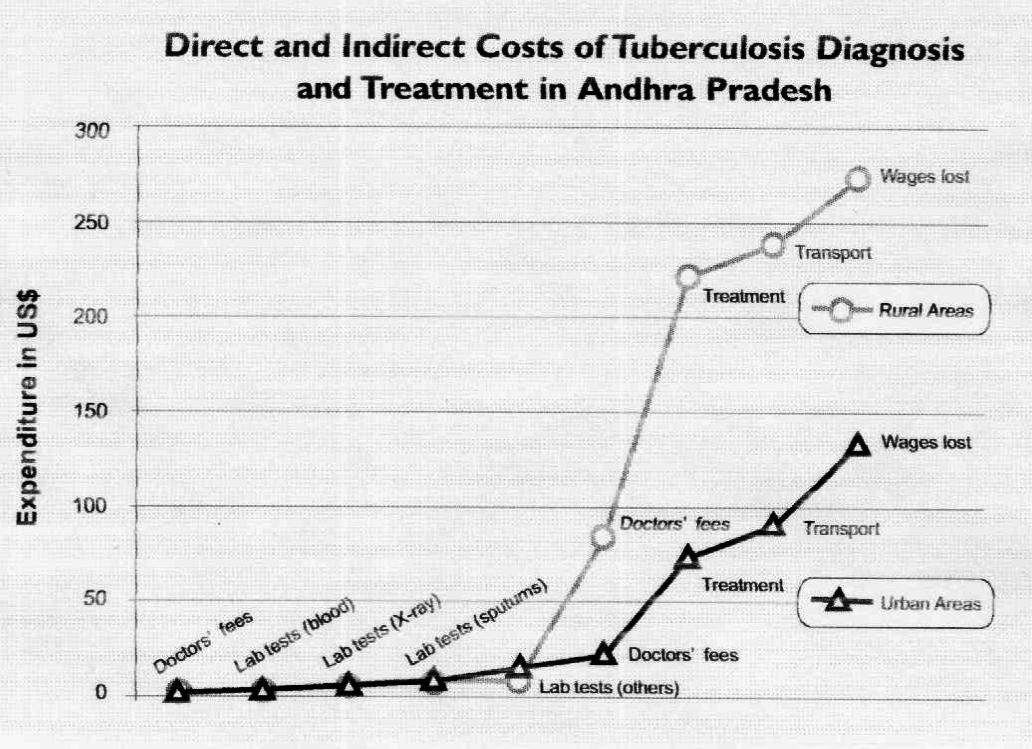
In
their study, Mapping of TB Treatment Providers at Selected Sites in Andra
Pradesh State, India, Ramana et al found that on average, rural tuberculosis
patients spent Rs 1000 ($30) per month on TB diagnosis and treatment while
urban patients spent Rs 500 ($15) per month (See figure). This almost
invariably resulted in indebtedness and mortgage of valuables.
The
World Health Organization estimates that TB patients in India together spent
more than Rs. 645 crore ($180 million) on private ŇÂ care in 1997.
Indian
workers with tuberculosis lost an average of 83 workdays because of the
disease, 48 of which were lost while shopping for diagnosis. Considering that
two million new cases are reported annually in India, the national loss per
year works out to 166 million lost workdays, at a cost of about $200 million
(Rs. 694 crore). In addition, the debts incurred by patients because of
tuberculosis amounted to $120 million (Rs. 416 crore).
ŇÂ kills more women of reproductive age than
all causes of maternal mortality combined, and it may create more orphans than
any other infectious disease. Nearly one third of female infertility in India
is caused by tuberculosis.
Indian
women who suffer from ŇÂ
face special constraints. They tend to neglect their illness due to household.
Responsibilities until they become too sick to attend to their normal duties.
They are often dependent on others to get necessary medical attention.
There
is also still a social stigma attached to TB. Sixty-nine percent of rural
females interviewed by TRC researchers were reluctant to discuss their illness
with neighbors.
The indirect
impact of TB on children is considerable. Two thirds of the women interviewed
in the Tamil Nadu study said that they were unable to look after the needs of
their children because of TB. Nearly one-fifth of the school-age children of TB
patients either left school or took up employment to help support their
families.
A
successful DOTS programme could have substantial economic benefits for India,
in his 1996 study, The Potential Economic Benefits of the DOTS Strategy Against
TB in India, R.H. Dholakia of the Indian Institute of Management, Ahmedabad,
divided these benefits into two broad categories.
Direct,
tangible economic benefits of DOTS would include:
●
Reduction in the incidence and prevalence of TB, which improves the
efficiency and productivity
Of workers by reducing their forced absenteeism on account of ill
health;
● TB
deaths averted, which adds to the productive capacity of the economy; and
●
Release of the hospital beds currently occupied by the TB patients.
In
addition, DOTS would enhance India's social welfare through:
●
Reduced suffering of TB patients,
●
Quicker and surer cure from the disease,
●
Lives saved and disability reduced for dependents and non-workers
suffering from TB,
●
Poverty alleviation, and
● The
benefits of living in a more healthy society.
HIV and TB
The Human
Immunodeficiency Virus (HIV) has spread across India since the first cases of
HIV infection were diagnosed in Bombay and Madras in 1986. WHO estimates that,
by 1999, at least 3 million, and possible as many as 5 million people in India
are infected with HIV, the virus that causes AIDS. That makes India the home of
more HIV-positive individuals than any other country in the world.
Because
the Human immunodeficiency Virus breaks down the immune system and makes
patients highly susceptible to TB, HIV will have 3 major impacts on the TB
epidemic in India. In some countries in Africa, the HIV epidemic has more than
doubled or tripled TB cases.
Infection
with HIV is the most potent known risk factor for progression to active
tuberculosis among adults. Conversely, tuberculosis hastens the development of
AIDS in HIV-infected persons. Individuals who are not HIV-infected and who
become infected with Mycobacterium tuberculosis have approximately a 10
percent lifetime risk of developing active tuberculosis, compared with a risk
of 60 percent or more in persons infected with both HIV and Mycobactenum tubercutosis.
The risk of tuberculosis infection progressing to active tuberculosis is
estimated to be 8 percent per year in an HIV-positive person, as opposed to a
Lifetime risk of 1O percent in an immunocompetent person. This is particularly
important in India where it is estimated that more than half of the adult
population harbors Mycobactenum tuberculosis infection.
In a developing country like India, the
potential extra burden of new tuberculosis cases attributable to HIV is
staggering and could overwhelm already stretched tuberculosis budgets and
support services.
The
incidence of HIV seropositivity among patients admitted to the tuberculosis
wards of a large public hospital in Bombay increased from 2% in 1988 to 16% in
1998. Among Indian patients who are HIV positive, tuberculosis is by far the
most common opportunistic infection. A 1994 study showed that 61 percent of all
HIV-positive patients in India had tuberculosis at some point in the course of
their HIV disease.
One
of the most worrisome aspects of the interaction between HIV and TB is that
strains of multidrug-resistant tuberculosis (MDRTB) can spread very rapidly
among HIV-infected persons. In both developed and developing countries,
outbreaks of MDRTB have spread rapidly on hospital wards for HIV-infected
persons.
Fortunately,
DOTS is as effective among HIV-infected TB patients as among those who are HIV
negative. Even among HIV-infected TB patients, DOTS cures patients and results
in longer, healthier lives.
Tanzania,
Malawi, and Botswana have had programmes of directly observed treatment for
more than 10 years. Despite high rates of HIV infection, which is present in
one third of tuberculosis patients or more, rates of relapse drug resistance
remain low.
Multidrug-Resistant
Tuberculosis (MDRTB)
Multidrug-resistant
tuberculosis refers to strains of tuberculosis bacteria that have developed
resistance to the two most effective anti-tuberculosis drugs available
-isoniazid and rifampicin. MDRTB is an eemerging and ominous problem worldwide.
Patients who do not have MDRTB can
Easily be cured with 6-9 months of treatment. In
contrast, treatment of MDRTB requires at least 18-24 months of arduous
treatment with expensive, often toxic, medications.
In the United States, treatment of a single case
of MDRTB can cost more than US$250,000. And, the treatment often fails. In a
country like India MDRTB is almost the equivalent of a death sentence, as very
few patients have the financial capacity or the stamina to complete the Song
treatment regimen required.
Effective
TB treatment programmes can prevent drug resistance. If patients are prescribed
appropriate treatment and complete that treatment, development of drug
resistance is extremely rare. In
contrast, when prescribing practices or case holding — or both — are
inadequate, drug resistance can emerge. Ensuring the cure of new smear-positive
patients is the best way to prevent the development of drug resistant
tuberculosis and should be the highest public health priority. A low cure rate
among new smear positive cases will create drug resistant cases faster than
these cases can be cured, even if unlimited resources are available.
Many of the
factors contributing to the development of drug resistance - poor patient compliance,
ineffective drug regimens, inadequate follow-up, and poor patient monitoring -
flourish in a developing country. DOTS
has been proven to prevent the emergence of MDRTB, and also to reverse it where
it has emerged. The only way to confront the challenge of MDRTB is to improve
the treatment programme and implement DOTS as rapidly as possible.
Key
Findings and implications for Action
Tuberculosis is the leading single infectious cause of
death in India. In addition to the negative health impact of tuberculosis, it
is a substantial economic burden for families and communities. The problems of
HIV and multidrug-resistance will make the tuberculosis epidemic much worse
unless urgent action is taken. But there is hope - tuberculosis can be cured
and the battle against the disease can be won.
• Policy-makers, programme managers, and doctors in public and
private sector should spread the message that TB can be cured and the epidemic
controlled. For too long, tuberculosis has been seen as a natural calamity
about which nothing can be done.
• Researchers and programme managers should promote much more
widespread awareness of the massive health, economic, and social costs of
tuberculosis - costs which could be greatly reduced by an effective programme.
• Policy-makers
should take into account the negative impact of TB on the economy of individual
families and of the country. Tuberculosis does not merely reflect
socio-economic status - tuberculosis perpetuates and exacerbates poverty
adequate funding for tuberculosis control is required at all levels.
• Policy-makers and programme managers should
recognize the serious risk that HIV infection and multidrug-resistant
tuberculosis can convert an already-serious situation into a massive and
potentially uncontrollable epidemic. It is essential that DOTS is rapidly and
effectively implemented before multidrug-resistant tuberculosis and HIV become
more widespread. However, implementation must be phased in order to ensure good
quality.
