
Photo Essay - February 1999
Corneal Changes Associated With Intrastromal Corneal Ring Segments
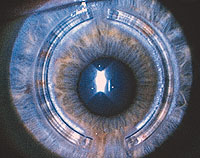
The cornea of an asymptomatic male patient was examined routinely 2 years after the implantation of intrastromal corneal ring (ICR) segments (Figure 1 and Figure 2).
|

|
| Figure 1.Ā
Intrastromal corneal ring segments in situ. I indicates epithelial iron ring; R,
ring segment; D, intrachannel deposits; and O, intrachannel opacification.
|
Figure 2. Ā Close
up of a section of a ring segment. I indicates epithelial iron ring; R, ring
segment; D, intrachannel deposits; and O, intrachannel opacification.
|
Ophthalmic examination revealed an intraepithelial concentric ring of iron deposition central to the segments. Along the central and peripheral borders of the ICR segments was a mild intrachannel opacification. Within the central area of intrachannel opacification were scattered white deposits that had a mixed crystalline/amorphous appearance.
COMMENT
The implantation of an ICR, and more recently ring segments of polymethylmethacrylate, is a procedure used to correct low degrees of myopia. It is thought to work by an "arc shortening" effect of the corneal lamellae, flattening the central cornea.[1] The procedure does not violate the visual axis and is reversible.[1] Short-term studies have shown good stability and predictability with few complications.[1,2]
Corneal epithelial iron deposition is found physiologically (Hudson-Stahli line) and adjacent to localized surface elevations. Previous reports in association with the ICR and ICR segments described inferior Hudson-Stahli line-type or arcuate deposition of iron.[2,3]
The intrachannel opacification has previously been referred to as "haze,"[1,2] but as this term tends to imply a healing/scarring process, it is probably inappropriate. It appears during the mechanical separation of corneal lamellae as the intralamellar keratome passes progressively through the corneal stroma dissecting a channel. This optical discontinuity persists between lamellae at the borders of the channel where the ICR segment does not fill the dead space. The opacification does not progress and may fade with time.
The white deposits are situated within the channel dead space along the central border, are not associated with any inflammatory or vascular response, and do not appear to be progressive, stabilizing after about 9 months. They probably represent lipid deposits in association with altered keratocytes.[1,2,4]
Fortunately, none of these corneal findings seems to have any visual consequence.
Andrew M. Fink, FRCOphth
Christa Gore MSc, MCOptom
Emanuel S. Rosen MD, FRCSE
Manchester, England
Ms Gore is a paid research coordinator for KeraVision, Fremont, Calif, manufacturers of the ICR. The other authors have no direct financial interest in the ICR.
Reprints: Emmanuel Rosen, MD, FRCSE, 10 St John St, Manchester M3 4DY, England (e-mail: Christa@eyes.u-net.com).
References
1. Schanzlin D, Asbell P, Burris T, Durrie D. The intrastromal corneal ring segments: phase II results for the correction of myopia. Ophthalmology. 1997;104:1067-1078.
2. Assil K, Barret A, Fouraker, Schanzlin D; for the Intrastromal Corneal Ring Study Group. One-year results of the intrastromal corneal ring in nonfunctional human eyes. Arch Ophthalmol. 1995;113:159-167.
3. Assil K, Quantock A, Barret A, Schanzlin D. Corneal iron lines associated with the intrastromal corneal ring. Am J Ophthalmol. 1993;116:350-356.
4. Parks RA, McCarey BE, Knight PM, Storie BR. Intrastromal crystalline deposits following hydrogelkeratophakia in monkeys. Cornea. 1993;12:29-34.
(Arch Ophthalmol. 1999;117:282)
® 1995-1999 American Medical Association. All rights reserved.