Jenny's Story: My Life with Crouzon Syndrome
Growing Up with Crouzon Syndrome
Being an Adult with Crouzon Syndrome
Being a Mother with Crouzon Syndrome
Dealing with Unexpected Crouzon Syndrome
Helping Your Child to Cope with Teasing
~~~~~
Jenny's Inspirational Sayings II
~~~~~


What is hydrocephalus?
The term hydrocephalus comes from the two Greek words: 'hydro' which means water, and 'cephalus' which means head. In years past, it was commonly called 'water on the brain'. Put simply it is a condition where there is too much cerebrospinal fluid in the cranium.
Cerebrospinal fluid (CSF) is found within the brain, and surrounds the brain and the spinal cord. It is a clear, watery substance. The fluid flows through a channel into the space around the brain and spinal cord, where it also functions as a cushion. The CSF is absorbed back into the bloodstream via mushroom-like structures over the brain called arachnoid villae, and replenished. A small amount of CSF is produced by the spinal cord. The CSF contains nutrients and proteins necessary for the nourishment and normal function of the brain and carries waste products away from tissues in and around the brain.
The fluid is produced within hollow channels in the brain called ventricles, primarily though within the lateral ventricle (see diagram below). In each ventricle is a specialized structure (which looks like small flower-like tufts) called the choroid plexus, which is responsible for the majority of CSF production. This production is at a constant rate. (The total volume of CSF is 125-150 ml. The normal resting pressure of the CSF is between 150-180 mm H2O. It has been calculated that 430 to 450 ml of CSF is produced daily.)

The brain normally maintains a balance between the amount of cerebrospinal fluid that is absorbed and the amount that is produced. Often, disruptions in the system occur.
Hydrocephalus occurs when there is an imbalance between the amount of CSF that is produced and the rate at which it is absorbed. This can be caused by a blockage in the pathways through which the fluid normally travels or from an overproduction of fluid or a difficulty in absorbing the fluid that is produced. Because the brain is enclosed within the bony skull, the extra fluid has no escape which causes it to build up. This then causes the ventricles to enlarge and the pressure inside the head to increase producing enlarged heads and increased pressure symptoms.
Types of hydrocephalus
Hydrocephalus can be congenital, when the condition exists at birth e.g. Spina Bifida, craniosynostosis syndromes etc, or acquired, when it occurs as the result of a head trauma, infection such as Meningitis, tumors or cysts after birth.
There are 4 types of hydrocephalus:
1) Noncommunicating or Obstructive hydrocephalus
There is an obstruction in the flow of CSF within the normal pathway.
2) Communicating or Non-obstructive hydrocephalus
There is no block in the flow of CSF, but the CSF is not absorbed properly back into the bloodstream.
3) Normal pressure hydrocephalus
Usually occurs in older age groups and is due to a lack of properly functioning brain structures.
4) Secondary hydrocephalus
Usually results from an infection (such as meningitis) or a severe head injury.
| Hydrocephalus is believed to occur in about 2 out of 1,000 births. |
Symptoms of hydrocephalus
| The most common symptoms are: increasing head size, extreme irritability, failure to feed and vomiting. |
There may be profound enlargement of the skull in infants because the immature skull is not yet fused (joined together) and expands to accommodate the excess fluid. In an older child or adult, the skull has fused and is quite rigid; therefore, fluid cannot enlarge the skull. Pressure may then increase in the brain due to the increase of fluid in the ventricles.
Other common symptoms include:
| headaches | |
| drowsiness and sleepiness | |
| confusion | |
| blurred vision | |
| motor and general developmental delay | |
| personality changes | |
| inability to concentrate | |
| failure to make appropriate visual and social contact | |
| fullness of anterior fontanelle | |
| splayed sutures | |
| scalp vein dilatation | |
| sunset eye sign and loss of upward gaze (upper eye lid retraction with defect of upward gaze and downward rotation of the globes) | |
| papilloedema |
For example:
| The infant may have developmental delays, such as delayed sucking, abnormal reflexes, sleepiness, fussiness, nausea or vomiting. | |
| The older child may complain of headaches, difficulty walking, nausea or vomiting, lack of energy, sleepiness, inattention, blurred vision or dizziness. | |
| In adult symptoms may consist of headaches, drowsiness, dizziness, nausea or vomiting, difficulty walking and visual changes. | |
| The elderly person often has symptoms of drowsiness, unsteady walking, loss of control of the bladder and confusion (or dementia). | |
| The elderly person may not complain of headaches as readily as the younger adult or child. |
Diagnosis of hydrocephalus
Hydrocephalus is diagnosed with the help of specialized tests such as:
| CT Scan (computerized axial tomography scan) which uses computer and x-rays to create a picture of the brain | |
| Ultrasound which uses high-frequency sound to create images of the brain | |
| MRI (magnetic resonance imaging) which produces three-dimensional images of the brain using powerful magnets and computer technology |
Treatment of hydrocephalus
The treatment of hydrocephalus depends on the cause. Some of the treatment options are: lumbar puncture, insertion of a shunt or removal of tumours.
1) Lumbar puncture is a temporary measure to drain some of the volume of CSF from the spinal canal. The skin around the lower back is cleansed with Betadine (or a surgical soap), and a local anesthetic (numbing medicine) is injected under the skin. A spinal needle then is inserted into the spinal canal, and a volume of CSF is drained out into a sterile container. The spinal needle then is removed and the puncture site closes on its own. This may be only a temporary measure or it may solve the problem until a more permanent solution is completed.
2) Insertion of a shunt is an operation in which a small catheter is placed from the ventricle to the abdomen, heart or gall bladder. The purpose of the operation is to provide an alternate path for the CSF to flow from the brain through the spinal canal. With a shunt in place, the CSF can flow through the normal pathway, which prevents large amounts from accumulating in the ventricle. Although the shunt is a permanent device, it may need to be surgically revised in the infant or child to accommodate for normal growth of the child. A shunt can be placed in a person of any age.
3) Tumours that are causing the obstruction may be able to be surgically removed.
Shunts
The most effective treatment is the surgical insertion of a device known as a ventriculoperitoneal shunt that can divert the excess CSF away from the ventricles in the brain to another area of the body. The place into which the CSF is usually diverted is the peritoneal cavity (the area surrounding the abdominal organs).
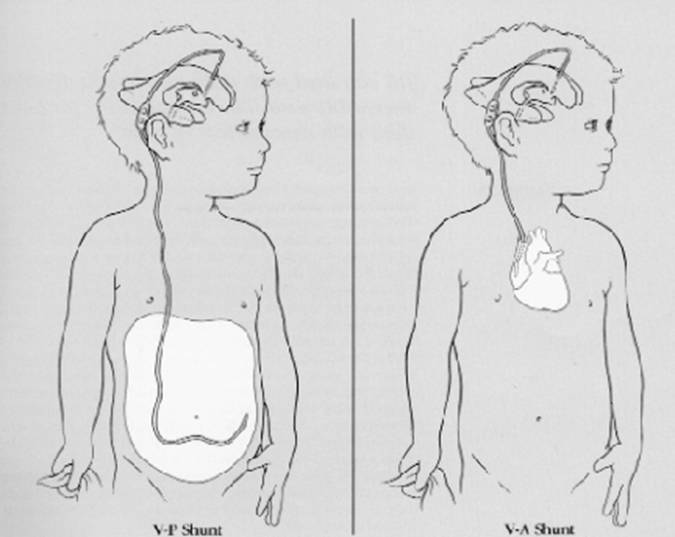
The shunt is a flexible tube that is inserted inside one of the ventricles in the brain. It diverts the flow of CSF into another region of the body where it can be absorbed. The tubing is threaded beneath the skin of the head, neck, chest or back and inserted into the peritoneal cavity, heart or gall bladder (see diagram below). The CSF can then be safely drained and absorbed into the bloodstream.
The shunt tube is about 1/8 inch in diameter and is made of a soft and pliable plastic that is well tolerated by the body's tissues. Shunt systems come in a variety of models but have similar functional components. Catheters (tubing) and a flow-control mechanism (one-way valve) are components common to all shunts. This valve allows CSF flow in a single direction (away from the brain) and maintains the CSF at normal pressure within the ventricles. The valve opens automatically when pressure exceeds a certain limit in the brain and allows CSF to drain.
The operation for inserting a VP Shunt
The surgical placement of a shunt, which is performed by a neurosurgeon, is a relatively short and uncomplicated procedure. The patient is brought to the operating room and is placed under general anesthesia. To insure cleanliness, a small region of the scalp may be clipped or shaved, and, for a ventriculoperitoneal (VP) shunt, the entire area from the scalp to the abdomen is scrubbed with an antiseptic solution.
The surgeon makes a small incision in the skin and a small hole through the skull bone, usually in the side or back of the right side of the head. The membranes between the skull and brain are opened. The ventricular end of the shunt is gently passed through the brain into the lateral ventricle. The shunt tube is passed beneath the skin, in the fatty tissue that lies just below the skin. After threading the tubing beneath the skin, a small incision is made in the lining of the abdomen and the abdominal (peritoneal) end is passed into the abdominal cavity. to place the tubing in the peritoneal cavity. This is where the CSF will ultimately be absorbed. The shunt system is completely inside the body. The incisions are then closed. When the procedure is completed, sterile bandages may be applied to the incisions and the patient is taken to the recovery room where the anesthesia is allowed to wear off.
Risks
Antibiotics are often prescribed for a short period of time to reduce the risk of infection. The hospital stay is usually short - one to two days after surgery. Certain risks must be considered with any surgery although the neurosurgeon takes every precaution to avoid complications. The most common risks with shunt surgery are infection, bleeding, malfunction, disconnection or obstruction. The sudden release of CSF during or after surgery can increase the risk for blood clots to form.
Problems with Shunts
| Shunt Infection |
Infection is a regular complication of the shunt operation and if left untreated can cause intellectual impairment. About 40% of shunt infections are caused by staphylococcus epidermidis and about 20% by staph aureus. Shunt infections usually present early after shunt insertion within eight to ten weeks. Symptoms include fever, headache and irritability with some neck stiffness.
| Mechanical failure |
The shunt can under drain or over drain. There can be a blockage of the catheter or the shunt valve can stop working or not work. The catheter can be improperly placed or the shunt system can migrate. The highest incidence of shunt failure occurs in the first few months after surgery.
| Shunt blockage |
It is estimated that 50% of mechanical shunt failure is due to shunt blockage. This is usually highest in the immediate post-operative period.
| Proximal occlusion |
Brain debris or parts of the choroid plexus can become attached to the pores of the proximal catheter and block it.
| Shunt valve blockage |
Brain debris or blood clots can be deposited within the valve system or the value system mechanism can stop working causing a blockage.
| Distal obstruction |
Particles can block the catheter in the peritoneal cavity. The catheter can also become isolated to one area leading to poor absorption. The catheter can also migrate outside the abdominal cavity or the abdominal wall. Catheters can also become disconnected and after a long time within the tissues they can become brittle and break.
Prognosis
The prognosis of hydrocephalus is determined by the cause, the presence of any other conditions, and the timeliness of diagnosis and treatment. Many infants and children treated for hydrocephalus are able to lead normal lives with few, if any, limitations. In some cases, the cause of the hydrocephalus leads to cognitive impairments, seizures or additional difficulties. Occasionally, if the shunt becomes infected or malfunctions, additional surgery may be needed.
Links:
http://www.neurosurgerytoday.org/what/patient_e/anatomy1.asp
http://www.hydroassoc.org/Default.htm
http://www.nlm.nih.gov/medlineplus/hydrocephalus.html