
KNEE
Jennifer Roberts
 PFPS is a broad term used to
describe any pain surrounding the front of the knee. This can be caused by several
different factors: softening of the cartilage beneath the kneecap (patella), abnormal
kneecap alignment, referred pain from another area such as the back or hip or from a
strain of the tendon that connects the kneecap to the lower leg bone (tibia), known as the
patellar tendon.
PFPS is a broad term used to
describe any pain surrounding the front of the knee. This can be caused by several
different factors: softening of the cartilage beneath the kneecap (patella), abnormal
kneecap alignment, referred pain from another area such as the back or hip or from a
strain of the tendon that connects the kneecap to the lower leg bone (tibia), known as the
patellar tendon.
In order to treat PFPS the cause of the problem must first be determined. If the cause of pain lies in the soft tissues such as the muscles, tendons or retinaculum, stretching is the recommended mode of therapy. A simple stretch that can be done to stretch out the front of the thigh is to lie face down, grab the affected side's ankle with one hand (or a looped towel/belt if you're unable to reach), and gently stretch the front of the knee. Remember, knee pain is not a good sign when stretching! Only apply enough stretch so that there is NO pain. More stretches.
If the cause is due to patellar alignment or misalignment then taping is a common form of treatment. In order to learn proper technique for this it is recommended that one seek a referral from their physician to a physical therapist. If taping is not effective, simply strengthening of the quadriceps muscles (front of the thigh) is strongly advised. Both strengthening and stretching are a good idea for anyone involved in sports, competitive or recreational.
Finally, symptomatic treatment is available with ice and non-steroidal anti-inflammatory drugs (
NSAIDs) available over-the-counter. Consult your physician on what medications are appropriate for you and the recommended dosage. Recommendations for ice.Along with the above treatments, limiting or modifying physical activities until the pain decreases is often helpful.
Although not a foolproof method, being in good overall physical condition is a big factor in avoiding such overuse injuries as well as acute injuries. Proper stretching and strength training without drastic increases in the stress on the front of the knee is crucial. Weight reduction and/or activity modifications may also be necessary in some individuals.
 Described as pain just below the patella
where the tendon connects it to the lower leg (tibia). Typically the pain can be
pinpointed to one spot and simply touching this area can cause terrible pain. The reason
for the name "jumper's knee" is because it was first described in the take-off
leg of high jumpers, however this is most prevalent in basketball players than anyone. If
your sport involves running and jumping you are susceptible as well.
Described as pain just below the patella
where the tendon connects it to the lower leg (tibia). Typically the pain can be
pinpointed to one spot and simply touching this area can cause terrible pain. The reason
for the name "jumper's knee" is because it was first described in the take-off
leg of high jumpers, however this is most prevalent in basketball players than anyone. If
your sport involves running and jumping you are susceptible as well.
The presentation of pain can be classified into four different phases:
Yes, you guessed it proper stretching and strengthening. In order to prevent irritation of the tendon it is essential to keep it stretched out so therefore you must stretch out the quadriceps muscle. Another common and easily correctable problem can be to strengthen the quadriceps as well, especially the vastus medialis (VMO). Weakness in this muscle can lead to alignment problems that cause the patella to drift to the right since it is not able to pull it medially (toward inside of knee) and keep it on track. You can tell if this is the cause of your pain by simply applying light pressure on the outside of your kneecap and pushing toward the inside of your knee. If the pain goes away you most likely have VMO weakness.
Along with the above suggestions, warming up well before activities (i.e. stretching),
icing after activities, taking NSAIDs and possibly wearing a neoprene knee sleeve, which can help with alignment of the patella, may be of benefit. This term is often misused and overused for various
conditions associated with the knee. It is actually defined as the "softening of the
cartilage" or "wear and tear" of the cartilage behind the kneecap.
Generally, the back of the patella is smooth articular cartilage. In this case, the
surface has become more like sandpaper.
This term is often misused and overused for various
conditions associated with the knee. It is actually defined as the "softening of the
cartilage" or "wear and tear" of the cartilage behind the kneecap.
Generally, the back of the patella is smooth articular cartilage. In this case, the
surface has become more like sandpaper.
The degeneration is typically a result of slow, subtle mechanical problems with knee extension that occur over many years of pounding and abusing the knee. It can also be caused by a direct force or fall onto your kneecap.
Symptoms of cartilage degeneration include pain near the inner portion of, or just below the patella. Pain is usually present after prolonged sitting with knees bent, (i.e. in a movie theater), running or walking down an incline or stairs.
This being a chronic degenerative injury, there is not much one can do on their own except to treat the symptoms of pain with ice and
NSAIDs and to limit the activity level. Consult a physician if you suspect this is what is causing your knee pain. There are some minor surgical procedures that can be done if the condition is severe and disabling enough.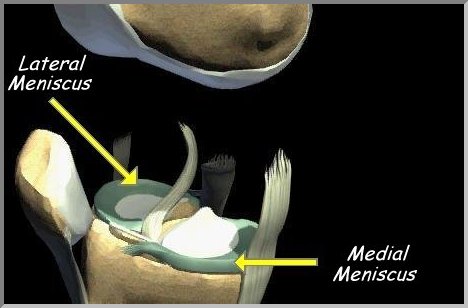 The knee contains 2 types of cartilage: articular and
fibrocartilage (meniscus). The articular cartilage is what covers the ends of the the two
large bones in the knee, the tibia and femur. This is responsible for cushioning and
protecting the bone. You are born with all the articular cartilage you will ever have and
once it's damaged it stays that way. The other type of cartilage is commonly known as
menisci, which are rings of dense, rubbery fibrous tissue that sit on top of the tibia and
act as "shock absorbers" between the two bones of the joint. They are attached
to the capsule that surrounds the joint and move with each action encounter- flexion,
extension, rotation. There are two menisci named based on their anatomical location:
medial and lateral. The key to protecting the articular cartilage is to keep the menisci
intact.
The knee contains 2 types of cartilage: articular and
fibrocartilage (meniscus). The articular cartilage is what covers the ends of the the two
large bones in the knee, the tibia and femur. This is responsible for cushioning and
protecting the bone. You are born with all the articular cartilage you will ever have and
once it's damaged it stays that way. The other type of cartilage is commonly known as
menisci, which are rings of dense, rubbery fibrous tissue that sit on top of the tibia and
act as "shock absorbers" between the two bones of the joint. They are attached
to the capsule that surrounds the joint and move with each action encounter- flexion,
extension, rotation. There are two menisci named based on their anatomical location:
medial and lateral. The key to protecting the articular cartilage is to keep the menisci
intact.
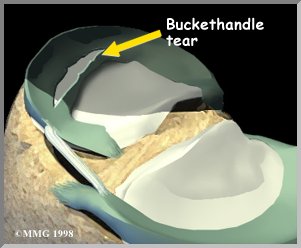 The medial meniscus, toward the midline, tears with
cutting-type maneuvers. Classically it is the football receiver who goes down the field,
plants his foot, cuts and then feels a snap in their knee. Afterwards they are unable to
straighten their knee all the way out. This type of tear is most likely to cause
"locking" of the knee.
The medial meniscus, toward the midline, tears with
cutting-type maneuvers. Classically it is the football receiver who goes down the field,
plants his foot, cuts and then feels a snap in their knee. Afterwards they are unable to
straighten their knee all the way out. This type of tear is most likely to cause
"locking" of the knee.
The lateral menisci usually tears upon weight bearing on a flexed (bent) knee. Common examples are a wrestler on bent knees on the mat, a dancer leaning backwards while her legs are bent underneath her to stretch, or simply squatting and inadvertently twisting a knee.
 Pain can be
pinpointed, not spread over the entire knee and swelling is not a necessity. In fact your
knee may be locking and have little evident swelling.
Pain can be
pinpointed, not spread over the entire knee and swelling is not a necessity. In fact your
knee may be locking and have little evident swelling.
The key to diagnosis is the mechanism of injury
(MOI). During the physical exam, the physician or physician assistant will perform a series of special tests that allow them to determine the extent of the cartilage damaged and can direct them towards their desired course of treatment.Depending on the severity, the meniscus may heal itself. However the majority don't because of their lack of blood supply and, therefore, need to be surgically repaired. This usually involves arthroscopic surgery to remove torn fragments, which if left alone would deteriorate the articular cartilage. How about life without those shock absorbers you ask? Yes, you will have less cushioning between the joint and your knee will wear out more quickly than if you had normal menisci, but not as fast as if you left the torn cartilage alone. Conclusion, see your PA or doctor!
 There are 4 basic ligaments that stabilize the
knee joint: the anterior cruciate, the posterior cruciate ligament, medial
There are 4 basic ligaments that stabilize the
knee joint: the anterior cruciate, the posterior cruciate ligament, medial
 The function of the
ACL is to control how far forward the tibia of shinbone moves in relation to the thigh
bone (femur). If the tibia shifts too far forward then the ACL can rupture. The most
common mechanism of injury
The function of the
ACL is to control how far forward the tibia of shinbone moves in relation to the thigh
bone (femur). If the tibia shifts too far forward then the ACL can rupture. The most
common mechanism of injury
The classic description of someone who has torn their ACL is that they planted their foot, turned and heard a "pop". There is usually immediate swelling (within a few hours) due to the bleeding inside the joint as a result of tearing surrounding blood vessels. Along with swelling there is associated pain, both of which typically resolve within 2-4 weeks. However, the patient may complain of instability or "giving way", especially when trying to change directions. The instability is what requires treatment and is usually addressed with surgical intervention in order to prevent long-term degeneration (i.e. arthritis) of the knee joint if the instability was not corrected.
The most important factor in diagnosing an ACL injury is by far the history and physical exam. The question of how the injury happened is very important in the diagnosis, especially in sports when someone plants, twists, and hears a "pop". This is in itself is almost enough to make a diagnosis. During the physical exam, the physician or physician assistant will perform a series of special tests that allow them to determine the laxity of the ligament and to
grade the severity of the tear. The presence of any swelling within 2-3 hours is considered by
orthopaedic surgeons to be due to bleeding in the joint, hemarthrosis. If swelling doesn't
occur until the next day it is probably due to the inflammatory response, not bleeding.
Draining some fluid off of the knee can be useful in diagnosis if blood is present in the
aspirated fluid. X-rays are generally taken to rule out fractures but know that ligaments
and tendons do NOT show up on x-rays. A more accurate type of imaging for
ligamentous injuries is the MRI (Magnetic Resonance Imaging). This is a painless,
non-invasive procedure but usually requires a few days to arrange and get the results back
plus it can be fairly expensive.
The presence of any swelling within 2-3 hours is considered by
orthopaedic surgeons to be due to bleeding in the joint, hemarthrosis. If swelling doesn't
occur until the next day it is probably due to the inflammatory response, not bleeding.
Draining some fluid off of the knee can be useful in diagnosis if blood is present in the
aspirated fluid. X-rays are generally taken to rule out fractures but know that ligaments
and tendons do NOT show up on x-rays. A more accurate type of imaging for
ligamentous injuries is the MRI (Magnetic Resonance Imaging). This is a painless,
non-invasive procedure but usually requires a few days to arrange and get the results back
plus it can be fairly expensive.
Initial treatment for an ACL injury includes crutches and rest until the swelling resolves. Once the swelling is gone, a physical therapist (PT) should be consulted to begin working on regaining normal range of motion and strength. Some physicians recommend wearing a brace to help with the instability during strenuous activity. If PT and bracing are ineffective, the most likely next step is reconstruction. This is when the surgeon will replace the torn ligament with a graft of choice. Your doctor can tell you more about the procedure itself if that is an option for you because each physician has their own preferences and minor differences. Following surgery, one can expect about 6 months of rehabilitation.

 The PCL, being one of the less
commonly injured ligaments of the knee, is not as advanced in treatment and research. The
function of the PCL is to control how far backwards the tibia (shinbone) moves in relation
to the femur (thigh). See anatomy.
The PCL, being one of the less
commonly injured ligaments of the knee, is not as advanced in treatment and research. The
function of the PCL is to control how far backwards the tibia (shinbone) moves in relation
to the femur (thigh). See anatomy.
The most common way that one tears their PCL is usually from a direct blow to the front
of the knee while the knee is bent (flexed), such as in an automobile accident. For this
reason, the injury is commonly called "dashboard knee". Other ways to injure the
PCL is while forcefully twisting or bending the knee too far backwards (hyperextending),
which typically happens when other ligaments are torn (i.e. ACL, MCL, etc).
As with any knee injury, symptoms will vary with each person and cause different functional limitations, depending on the strength and stability of the other surrounding ligaments and muscles in the knee. There may or may not be swelling with a PCL injury because of its location outside of the knee joint, in contrast to an ACL injury where there is swelling within hours of the injury. Any pain and swelling will usually resolve within 2-4 weeks of injury but the instability remains and is especially noticeable when trying to change directions.
Much like an ACL injury, the history and physical exam are the key to diagnosing the PCL injury. In the exam, the physician or physician assistant will perform a series of special tests that allow them to determine the laxity of the ligament and to
grade the severity of the tear. X-rays may be ordered to rule out any fractures but remember ligaments and tendons won't show up on x-rays. The MRI is a more accurate, more expensive method of imaging that shows soft tissues of the body.The first goal of treating a PCL injury is to limit the swelling and pain and this can be done immediately following the injury with
ice. Depending on severity, a long-leg brace and crutches may be recommended to help protect the knee form any additional trauma/stress while also decreasing the pain. Next, physical therapy will be started to continue towards your first goal and to regain full range of motion (ROM) and strength, especially of the quadriceps. Closed kinetic chain exercises are increasingly popular among therapists and are easy and effective for quadriceps strengthening. They are easy to do without any equipment and are considered functional because they mimic activities of daily living. For less severe tears, a progressive rehabilitation is usually the extent of the treatment, while for more severe tears surgery may be required. The key to successful non-surgical treatment is to provide long term control of swelling, giving way, and pain. However, activity modifications may need to be made to limit pivoting, cutting and jumping.
 Tears of the
collateral ligaments often occur when the lower leg is forced sideways, either away from
the other leg (lateral) or towards the opposite knee (medial). A blow to the outside of
the knee while the foot remains planted commonly results in a tear of the MCL. Other than
the common sports-related causes, many people injure these ligaments by simply slipping on
ice or water spot, etc. and this causes the foot and lower leg to slip outwards, stressing
the MCL.
Tears of the
collateral ligaments often occur when the lower leg is forced sideways, either away from
the other leg (lateral) or towards the opposite knee (medial). A blow to the outside of
the knee while the foot remains planted commonly results in a tear of the MCL. Other than
the common sports-related causes, many people injure these ligaments by simply slipping on
ice or water spot, etc. and this causes the foot and lower leg to slip outwards, stressing
the MCL.
As a result of the significant trauma required to tear one of the collateral ligaments, there is usually bleeding into the tissues around the knee, swelling of the tissues and possible bleeding into the knee joint itself. The knee will be stiff and painful and as a result, may feel unstable and give way.
The physical exam can give a good indication as to what ligaments have been torn in and around the knee. Sometimes this requires waiting 5-7 days after an injury to let the swelling and pain resolve before performing a thorough exam. In the exam, the physician or physician assistant will perform a series of special tests that allow them to determine the laxity of the ligament and to
grade the severity of the tear. Along with these "special tests", x-rays can be used to rule out damage to bone but a special type of x-ray known as a "stress x-ray" can actually confirm a torn collateral ligament. It's just like a plain x-ray but someone attempts to open the suspected unstable side of the joint by applying "stress". The x-rays reveal a widening of the joint space on the side where the instability exists. Of course the MRI will show evidence of all the soft tissues damaged including the all ligaments and any injury to the meniscus.Most isolated collateral ligament injuries do not require surgical intervention and usually heal on their own with simple immobilization or bracing for 4-6 weeks. Initial treatment involves decreasing the inflammation/swelling and controlling the pain in the knee with ice and
NSAIDs. As the ligament starts to heal, after a few weeks, physical therapy can be started and this will continue to manage the pain and inflammation while also improving range of motion and regaining strength. The exercises you will be given to regain motion and strength will be progressive and must be gradually implemented to assure no further aggravation. Closed kinetic chain exercises are increasingly popular among therapists and are easy and effective for quadriceps strengthening. They are easy to do without any equipment and are considered functional because they mimic activities of daily living.Questions on web page content matters - email Jennifer @ jlrobert@ufl.edu
Questions on weg page technical matters - email Mike @ florthopa@yahoo.com
