New Method of Herniorrhaphy Without Mesh
New method of inguinal hernia repair: A new solution
ANZ Journal of Surgery 71 (4), 241-244
(Live operation on direct, indirect &
recurrent groin hernia operations in a CD for $ 50)
Correspondence
Dr M. P.
Desarda,
18 Vishwalaxmi Housing Society, Kothrud,
Pune 411 029,
Email: mailto:desarda@gmail.com
Dr.Desarda Mohan P. Department of Surgery, Bharati Vidyapith (Deemed
University)
Background
A new technique to strengthen the posterior wall of the inguinal canal
in all types of inguinal hernias is described. This method of repair is done
without mesh and has been developed because mesh is not easily available in
rural or remote parts of many countries.
Method
After excision of the sac, a strip of the external oblique aponeurosis
(EOA) is partially separated from its medial leaf, keeping its continuity
intact at either end. This undetached strip of EOA is sutured to the inguinal
ligament below and the arch of muscle above, behind the cord, to form a new
posterior wall. This strip is put under tension by muscular contraction and
works as a shield to prevent recurrence so that the external oblique muscle
gives additional strength to the weakened internal oblique and transverse
abdominis muscles.
Results
A total of 400 patients have been operated on from 1983 to 1999 and
follow up by physical examination was carried out. (Eighty patients have been
followed up for more than 10 years.) The postoperative period was
comfortable with a hospital stay of 2–3 days and a return to work within
1–2 weeks. Recurrence was seen in only one case and haematocoele in one
case.
Conclusion
These results are comparable with operations performed with mesh. This
operation is simple to perform, does not require mesh or extensive dissection
and has produced excellent results. Therefore it is a good alternative to mesh
or other open or laparoscopic repairs.Key words: hernia, herniorrhaphy,
inguinal hernia, strip of external oblique aponeurosis.
Classical operations described by Bassini, McVay, Shouldice or others
require expertise in hernia surgery to carry out the complicated and risky
dissection of the inguinal floor and to identify and suture Cooper’s ligament
or the iliopubic tract. The recurrence rate in inguinal hernia surgery
performed by expert hernia surgeons or carried out in centres with a special
interest in such repairs is < 2%; but in the hands of average or junior
surgeons the reported recurrence rate is as high as 25%.1–6 This is
probably because the majority of them perform a modified Bassini or modified
Shouldice procedure in order to avoid the complicated and risky dissections,
instead of the classical operations described by the original authors.The
requirement of this group of surgeons is not to find an operation that converts
recurrence rates from 2 to 1% in the hands of experts, but to find an operation
that is simple, easy to perform, does not require extensive dissection or use
of a foreign body such as a mesh, and which also gives a recurrence rate of
< 2% without any major complications during or after surgery,
especially because they are all operating in less than ideal conditions.The
present series of hernia operations, using a strip of external oblique
aponeurosis (EOA) in place of a mesh prosthesis, assumes importance because the
technique can be performed by any general surgeon without expertise in hernia
surgery and it reduces the cost incurred in the use of a mesh. The availability
of mesh prostheses in smaller towns in underdeveloped countries is also a major
problem. Further, this operation technique is very simple and safe; it is easy
to understand and at the same time it has shown excellent results with a
virtually zero recurrence rate.
Four hundred cases of inguinal hernia were operated on in the period
between February 1983 and July 1999. All patients were between the ages of 18
and 90 years and 82% of patients were in the 30–80-year age group. The
types of hernia in these patients are listed in Table 1. A total of 371
patients received spinal anaesthesia, 26 received local anaesthesia and three
patients received general anaesthesia. No patient selection was used for the
surgical procedure and cases with bilateral hernia were operated on both sides
at the same sitting. Additional surgical problems such as hydrocele, piles,
enlarged prostate and varicocele were also dealt with at the same time whenever
required. Ambulation was permitted from the day of surgery and normal activity
was permitted after a week. The majority of patients (85%) required a hospital
stay of 3–4 days only. Eleven per cent of patients required a stay of
5–7 days and 4% required a stay of more than 7 days. Sutures were
removed on the 8th day. Ampicillin and Cloxacillin and diclofanac were given
for a week as prophylaxis because of the possibility of poor hygienic
conditions at the residence. Follow up of operated cases was done after 15 days,
1, 2, 3 months and then every year. Physical examination was insisted upon
but a correspondence option was also used. Ninety-nine per cent of patients
returned for a follow-up visit after 15 days, 85.6% returned after 1, 2
and 3 months; 61.2% of patients presented at the 1-year follow up, 58.3%
presented at the 2-year follow up, 53.5% presented after 3 years, 40.5%
presented after 5 years, 35.6% presented at the 7-year follow up and 26.6%
patients came for follow up for more than 10 years. The author is aware
that a 10-year follow up of 26.6% is not enough, but this is not a sufficient
reason for ignoring the results of the present series. Publication of these
data may encourage others to conduct more trials to prove or disprove these
results.
Skin and fascia are incised through a regular oblique inguinal incision
to expose the EOA. The thin and glistening, filmy fascial layer covering the
EOA is kept undisturbed as far as possible and an assessment made about the
strength of the EOA and its thinned-out portion. The thinned-out portion is
usually seen at the top of the hernia swelling, extending and fanning out to
the lower crux of the superficial ring. The EOA is cut in line with the upper
crux of the superficial ring. This leaves the thinned-out portion in the lower
leaf and a good strip can be taken from the upper leaf. The EOA, which is
thinned out due to ageing or longstanding large hernias, can also be used for
repair if it is able to hold the interrupted sutures.The cremasteric muscle is
incised for the herniotomy, and the spermatic cord along with the cremasteric
muscle is separated from the inguinal floor. Excision of the sac is done in all
cases except in small direct hernias where it is inverted.The medial leaf of the
EOA is sutured with the inguinal ligament from the pubic tubercle to the
abdominal ring using 1–0 Ethilon or Prolene interrupted sutures. The first two
sutures are taken in the anterior rectus sheath where the EOA is fused with it.
The last suture is taken so as to sufficiently narrow the abdominal ring
without constricting the spermatic cord (Fig. 1). Each suture is passed
first through the inguinal ligament, then the transversalis fascia and then the
EOA. The index finger of the left hand is used to protect the femoral vessels
and retract the cord structures laterally while taking lateral sutures.A
splitting incision is taken in this sutured medial leaf of the EOA, partially
separating a strip with a width equivalent to the gap between the muscle arch and
the inguinal ligament. This splitting incision is extended medially up to the
pubic symphisis and laterally 1–2 cm beyond the abdominal ring. The medial
insertion and lateral continuation of this strip is kept intact. A strip of the
EOA is now available, the lower border of which is already sutured with the
inguinal ligament. The upper free border of the strip of the EOA is now sutured
to the internal oblique or conjoined muscle lying close to it with 1-0 Ethilon
or Prolene interrupted sutures throughout its length (Fig. 2). The
aponeurotic portion of the internal oblique muscle is used for suturing to this
strip wherever and whenever it is possible, avoiding tension, but it is not
important to the success of the operation. This will result in the strip of EOA
being placed behind the cord to form a new posterior wall of the inguinal
canal. At this stage the patient is asked to cough and the increased tension on
the strip exerted by the external oblique to support the weakened internal
oblique and transverse abdominis is clearly visible. This increased tension
exerted by the external oblique muscle is the essence of this operation. The
spermatic cord is placed in the inguinal canal and the lateral leaf of the EOA
is sutured to the newly formed medial leaf of the EOA in front of the cord, as
usual, again using 1–0 Ethilon or Prolene interrupted sutures. Undermining of
the newly formed medial leaf of the EOA on both of its surfaces facilitates its
approximation to the lateral leaf. The first stitch is taken between the
lateral corner of the splitting incision and lateral leaf of the EOA. This is
followed by closure of the superficial fascia and the skin as usual.
Six patients exhibited swelling in the operated area during the postoperative
period; this subsided on its own without any treatment within a couple of
weeks. This was possibly due to the venous congestion caused by extra narrowing
of the internal ring during surgery. Four patients had mild skin infection that
subsided within 1 week. One patient developed a haematocele, which was
drained. No other complications (such as severe postoperative pain, major
infection, testicular atrophy etc.) were seen. Only one patient who was
operated on in 1984 suffered from recurrence of hernia after 2 years.
There was no other case of recurrence or late complications reported.
Reoperation on this patient revealed a healthy strip of EOA without any
necrosis, and fusion with the inguinal ligament and the muscle arch was good
without any fibrous adhesions tosurrounding structures. All patients were
ambulatory with limited movement from the second day, and 89% were ambulatory
with free movement in 4 days. Eighty-five per cent of patients were
discharged on the 3rd or 4th day and the median hospital stay was
3.5 days. No patient had severe pain that restrained movement during the
hospital stay or later. Ninety-six per cent of patients had mild pain for
2–4 days that did not restrict free movement. All patients were able to
return to their routine work within 1–2 weeks.
Ninety per cent of patients in this series were kept in the hospital
from 3 to 5 days for observation following operation. The author,
encouraged by the results, is confident about converting this procedure to
day-stay surgery. Similarly, the majority of patients were given spinal
anaesthesia only to perform the technique smoothly and watch for further
improvements if any. Now the majority of patients are operated on under local
anaesthesia only.
Since its original description in 18877 Bassini’s operation
has become a standard for inguinal hernia repair. Since then there have been
many modifications to this repair, predominant being those described by
Halsted, McVay and Shouldice. These techniques share the same principle of
pulling down the internal oblique and transverse abdominis muscle to suture
with either the inguinal or Cooper’s ligament or the iliopubic tract. There
were three objections raised regarding these open operations: (i) Halsted was
one of many authors who criticized and warned of the danger of tension on the
suture line and stated ‘no tension’ as one of the great principles of surgery;8
(ii) these authors advised incision/excision of the transversalis fascia
requiring extensive dissection; and (iii) Amid et al. reported that
the use of already weakened muscles and transversalis fascia, especially under
tension, is a violation of the most basic principles of surgery.9
Hay et al. compared Shouldice to Bassini and Cooper’s ligament
repair and found that, in a study of 1578 hernias at an average of
8.5 years follow up, the recurrence rate was 6% compared to a recurrence
rate of 8.6% using Bassini and a recurrence rate of 11% using Cooper’s ligament
repair.10 Panos et al. and Kingsnorth et al.
have stated that the recurrence rates from smaller institutions and general
ordinary surgeons seem, in the literature, to be worse than those from
specialist centres such as Shouldice or Lichtenstein clinics.5,6 Obviously
those open hernia operations described by the original authors do not satisfy
all the criteria of modern hernia surgery, and modifications of those
operations failed to give the desired results especially in the hands of junior
surgeons.Therefore, more recently, the use of a mesh prosthesis for inguinal
hernia repair has been quite popular among general surgeons worldwide. The
operation described by Lichtenstein is simple and safe and achieves all the
goals of modern hernia surgery.11 But the mesh prosthesis has its
own drawbacks. First, it is not available in every part of the world. Second,
it increases the cost of the operation. Third, because the groin is a mobile
area there is a tendency for the mesh to fold, wrinkle or curl. Mesh prostheses
lose approximately 20% of their size, in vivo, through shrinkage. The
slightest movement of the mesh from the sutured area, due to the aforementioned
factors, is a leading cause of failure of mesh repair of inguinal hernias.12
Further, chronic groin sepsis following mesh repair is more frequent than
reported previously and complete removal of mesh is required to treat this
condition.13The ageing process is minimal in the tendons and
aponeurosis. Therefore the use of a strip of EOA, which is tendo-aponeurotic in
nature, is the best alternative to a mesh or Shouldice. The thinned out portion
of the EOA was also used by the author with good results. This eliminates all
the drawbacks and complications of using a foreign body such as a mesh, and
also avoids extensive, complicated dissections. The author’s technique
satisfies all the criteria of modern hernia surgery. It is simple and easy to
perform and learn. Even a junior resident can easily operate by this technique.
It does not require complicated and risky dissection or suturing. There is no
tension on the suture line. It does not require any foreign material such as
mesh nor does it use weakened muscles or transversalis fascia for repair. Even
suture material like prolene or ethilon, used by the author, can be replaced by
any other suitable suture material. The results of the present series have
demonstrated a minimum hospital stay in 90% of patients. All patients were
ambulatory on the second day. A total of 96% of patients had a very comfortable
postoperative period with minimal pain. Ninety-nine per cent of patients had a
rapid recovery and they were able to return to work in 1–2 weeks. This
operation is cost-effective and early or late complications are well below
1–2%.Suturing of the EOA behind the cord and the use of a detached strip of EOA
or fascia lata for darning purposes has been described. Double breasting of the
EOA was done by Zimmerman for repairs of inguinal hernias.14 In
Andrew’s imbrication operation15 the entire medial leaf of the EOA
along with the internal oblique and transverse abdominis muscle is sutured to
the inguinal ligament behind the cord, and the lateral leaf of the EOA is used
to cover the spermatic cord in front. The author’s operation differs from the
Andrews technique because the procedure of strengthening the posterior wall of
the inguinal canal is different and the mechanism of action involved to prevent
reherniation is also different. The author did not find any technique in the
medical literature similar to the one described here.
Contraction of the external oblique muscle creates lateral tension in
this strip while contraction of the internal oblique/conjoined muscle pulls
this strip upwards and laterally against the inguinal ligament, creating tension
above and laterally and turning the strip into a shield to prevent any
herniation. This additional strength given by the external oblique muscle to
the weakened muscle arch to create tension in the strip and prevent
reherniation is the essence of this operation. The shielding action of the
strip of EOA can be elegantly demonstrated on the operating table by asking the
patient to cough. The much publicized shutter mechanism, to prevent herniation,
is already lost once a hernia is formed. It is the shielding action of the
abdominal muscles, or their aponeurotic extensions, that is the main factor in
preventing the herniation. The transversalis fascia acts as a barrier to
prevent hernia because it is supported in the posterior wall of the inguinal
canal by aponeurotic extensions from the muscle arch. If those aponeurotic
extensions are absent and the transversalis fascia is weak then the use of the
transversalis fascia at any stage of repair should be redundant. In this
operation the weakened transversalis fascia is supported by the shielding
action of this strip of the EOA on the posterior wall of the inguinal canal, in
place of absent aponeurotic extensions, and therefore the possibility of
herniation behind this strip, through the transversalis fascia, is also
removed.
1. Kux M, Fuchsjager N, Schemper M. Shouldice is superior to
Bassini inguinal herniorrhaphy. Am. J. Surg. 1994; 168: 15–18.
2. Berliner S, Burson L, Katz P, Wise L. An anterior transversalis
repair for adult inguinal hernias. Am. J. Surg. 1978; 135: 633–6.
3. Piper JV. A comparison between whole thickness skin graft and
Bassini methods of repair of inguinal hernias in men. Br. J. Surg. 1969;
56: 345–8.
4. Belanger J, Flament JP, Goldstein M. Bilan de 14 annees de
oures de hernies. Acta Chir. Belg. 1975; 60: 37–9.
5. Panos RG,
6. Kingsnorth AN, Gray MR, Nott DM. Prospective randomized trial
comparing the Shouldice technique and plication darn for inguinal hernia. Br.
J. Surg. 1992; 79: 1068–70.
7. Brown RK, Galleti G, Tumm KS. New technique for the cure of inguinal
hernia: By Edoardo Bassini in 1887 to 1890. J. Hist. Med. Allied Sci.
1966; 21: 401–7.
8. Halsted WS. The radical cure of inguinal hernia in the male. Bull.
Johns
9. Amid PK, Shulman AG, Lichtenstein L. Femoral hernia resulting
from inguinal herniorrhaphy: The ‘plug’ repair. Contemp. Surg. 1991; 39:
19–24.
10. Hay JM, Boudet MJ, Fingerhut A et al. Shouldice
inguinal hernia repair in the male adult: The gold standard? A multicentral
controlled trial in 1578 patients. Ann. Surg. 1995; 222: 719–27.
11. Shulman AG, Amid PK, Lichtenstein IL. A survey of non-expert
surgeons using the open tension free mesh patch repair for primary inguinal
hernias. Int. Surg. 1995; 80: 35–6.
12. Amid PK,
13.
14. Zimmerman LM. Recent advances in surgery of inguinal hernia. Surg.
Clin. North Am. 1952; 32: 135–54.
15. Wyllys Andrews operation
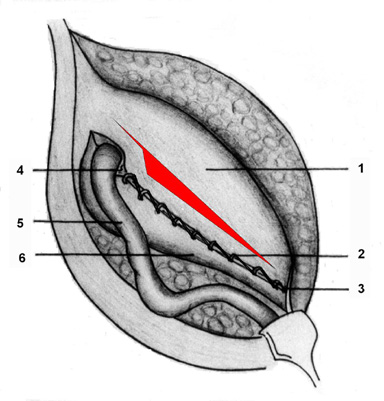
Fig. 1. The medial leaf of the external oblique aponeurosis
(EOA) is sutured to the inguinal ligament. 1, medial leaf of EOA; 2,
interrupted sutures taken to suture the medial leaf of the EOA to the inguinal
ligament; 3, pubic tubercle; 4, abdominal ring; 5, spermatic cord; 6, lateral
leaf of the EOA.
Fig. 2. Undetached strip of external oblique
aponeurosis (EOA) forming the posterior wall of the inguinal canal. 1,
reflected medial leaf of the EOA after a strip is separated; 2, internal
oblique muscle seen through the splitting incision taken in the medial leaf of
the EOA; 3, interrupted sutures between the upper border of the strip and
conjoined muscle/internal oblique muscle; 4, interrupted sutures between the
lower border of the strip and the inguinal ligament; 5, pubic tubercle; 6,
abdominal ring; 7, spermatic cord; 8, lateral leaf of the EOA.
Table 1. Inguinal hernia types
Hernia
type
No. cases (%)
Direct
100 (25.00)
Indirect
297 (74.25)
Pantaloon
hernia
3 (0.75)
Obstructed
15 (3.75)
Recurrent
16 (4.00)
Right side
hernia 216
(54.00)
Left side
hernia
125 (31.25)
Bilateral
59 (14.75)
(Click here to see image)
FIG.1. Medial leaf of EOA is sutured to the inguinal
ligament with splitting incision taken
1=Medial leaf; 2=Continuous absorbable sutures taken
to suture the medial leaf to the inguinal ligament; 3=Pubic tubercle;
4=Abdominal ring; 5=Spermatic cord; 6= Lateral leaf.
(Click here to see image)
FIG.2. Undetached strip of external oblique aponeurosis
forming the posterior wall of inguinal canal.
1=Reflected medial leaf after a strip has been separated;
2= Internal oblique muscle seen through the splitting incision made in the
medial leaf; 3= Continuous absorbable sutures between the upper border of the
strip and conjoined muscle or internal oblique muscle; 4= Continuous absorbable
sutures between the lower border of the strip and the inguinal
ligament; 5=Pubic tubercle; 6= Abdominal ring; 7=Spermatic cord; and 8=
Lateral leaf.
BUY A CD FOR JUST $ 50 ONLY
(Live operation on direct, indirect & recurrent groin hernia)
EMAIL: desarda@gmail.com
{kind=link}
{kind=link}