OPERATION
TECHNIQUE
Skin and fascia are incised through a regular oblique inguinal incision to expose
the external oblique aponeurosis. The thin, filmy fascial layer covering it is
kept undisturbed as far as possible and an assessment made about the strength
of it and its thinned-out portion. The thinned out portion is usually seen at
the top of the hernia swelling, extending and fanning out to the lower crux of
the superficial ring.
The external oblique is cut in line with the upper crux of the superficial
ring, which leaves the thinned out portion in the lower leaf so a good strip
can be taken from the upper leaf. The external oblique, which is thinned out as
a result of aging or long standing large hernias, can also be used for repair
if it is able to hold the interrupted sutures. The cremasteric muscle is
incised for the herniotomy and the spermatic cord together with the cremasteric
muscle is separated from the inguinal floor. The sac is excised in all cases
except in small direct hernias where it is inverted. The medial leaf of the
external oblique aponeurosis is sutured with the inguinal ligament from the
pubic tubercle to the abdominal ring using PDSII no.1 (Monofilament Polydioxanone violet, Ethicon)
continuous sutures. The first
two sutures are taken in the anterior rectus sheath where it joins the external
oblique aponeurosis. The last suture is taken so as to narrow the abdominal
ring sufficiently without constricting the spermatic cord (Figure 1). Each suture
is passed first through the inguinal ligament, then the transversalis fascia,
and then the external oblique. The index finger of the left hand is used to
protect the femoral vessels and retract the cord structures laterally while
taking lateral sutures.
A splitting incision is made in this sutured medial leaf, partially separating
a strip with a width equivalent to the gap between the muscle arch and the
inguinal ligament but not more than 2 cms. This splitting incision is extended
medially up to the pubic symphisis and laterally 1–2 cms beyond the abdominal
ring. The medial insertion and lateral continuation of this strip is kept
intact. A strip of the external oblique, is now available, the lower border of
which is already sutured to the inguinal ligament. The upper free border of the
strip is now sutured to the internal oblique or conjoined muscle lying close to
it with PDSII no.1
(Monofilament Polydioxanone violet, Ethicon) continuous sutures throughout its length (Figure 2). The aponeurotic
portion of the internal oblique muscle is used for suturing to this strip
wherever and whenever possible to avoid tension; otherwise, it is not a must
for the success of the operation. This will result in the strip of the external
oblique being placed behind the cord to form a new posterior wall of the
inguinal canal.
At this stage the patient is asked to cough and the increased tension on the
strip exerted by the external oblique to support the weakened internal oblique
and transversus abdominis is clearly visible. The increased tension exerted by
the external oblique muscle is the essence of this operation. The spermatic
cord is placed in the inguinal canal and the lateral leaf of the external
oblique is sutured to the newly formed medial leaf of the external oblique in
front of the cord, as usual, again using PDSII no.1 (Monofilament Polydioxanone violet, Ethicon)
continuous sutures. Undermining
of the newly formed medial leaf on both of its surfaces facilitate its
approximation to the lateral leaf. The first stitch is taken between the
lateral corner of the splitting incision and lateral leaf of the external
oblique. This is followed by closure of the superficial fascia and the skin as
usual.
(Click here to see image)
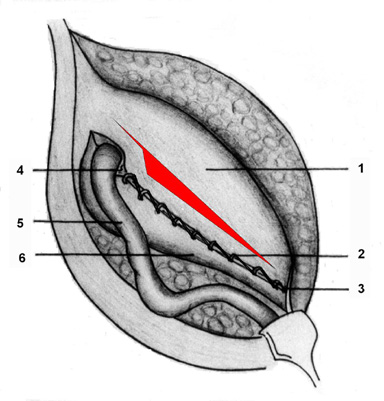
FIG.1. Medial leaf of EOA is sutured to the inguinal
ligament with splitting incision taken
1=Medial leaf; 2=Continuous absorbable sutures
taken to suture the medial leaf to the inguinal ligament; 3=Pubic tubercle;
4=Abdominal ring; 5=Spermatic cord; 6= Lateral leaf.
(Click here to see image)
FIG.2. Undetached strip of external oblique aponeurosis
forming the posterior wall of inguinal canal.
1=Reflected medial leaf after a strip has been
separated; 2= Internal oblique muscle seen through the splitting incision made
in the medial leaf; 3= Continuous absorbable sutures between the upper border
of the strip and conjoined muscle or internal oblique muscle; 4= Continuous
absorbable sutures between the lower border of the strip and the inguinal
ligament; 5=Pubic tubercle; 6= Abdominal ring; 7=Spermatic cord; and 8=
Lateral leaf.
BYE A CD FOR JUST $ 20 ONLY
(Free to medical
professionals)
(Live operation on
direct, indirect & recurrent groin hernia)
EMAIL: desarda@gmail.com
WEB SITE: http://www.oocities.org/desarda
{kind=link}
{kind=link}