Physiological repair of inguinal hernia-A
new technique (Study of 860 patients)
Hernia.
(2006) 10:143-146
(Hernia-The world journal of abdominal wall
surgery, 2006)
Dr.
M. P. Desarda
M.S. (Gen.Surg.)
1.
2.
3. Dr. Desarda Nursing Home
Address for correspondence
Dr. M. P. Desarda,18,
Vishwalaxmi housing society, Kothrud, Pune – 411 029 (
E MAIL: desarda@gmail.com Telephone: +91 20 32905343
ABSTRACT
INTRODUCTION: The author has
developed a new operation technique based on physiological principle that
provides dynamic posterior wall for inguinal hernia repair. Results of the
first series of 400 patients were published in 2001.[1] Now the
author has described the results of second series of 860 patients having 920
hernias with follow up for more than 7 years.
METHODS: An un-detached strip of
the external oblique aponeurosis (EOA) is sutured to the inguinal ligament
below and the muscle arch above, behind the cord, to form a new posterior wall.
External oblique muscle gives additional strength to the weakened muscle arch
to keep this strip physiologically dynamic. In this prospective study, 920
inguinal hernia repairs were performed between August 1990 and December 2003 in
860 patients. Follow up was done for 7 years. The main outcome measure was
early and late morbidity and especially recurrence in a long term follow up.
RESULTS: Mean patient age was 50.5
years (range, 18 – 90). 851 (98.95%) patients were operated under local or
regional anesthesia. 838 (97.4%) patients were ambulatory with limited
movements in 6 hours and free movements in 18-24 hours. 792(92%) patients had a
hospital stay of one night and 840(97.6%) patients returned to normal activities
within 1-2 weeks. Hematoma formation requiring drainage was observed in 1
patient, while seven patients had wound oedema during the postoperative period
which subsided on its own. Follow-up was completed in 623 patients (72.5 %) by
clinical examination or questionnaire. The median follow-up period was 7.8
years (range, 1 – 12 years). There was no recurrence of the hernia or
postoperative neuralgia.
CONCLUSIONS: This operation is
simple to perform, does not require foreign body like mesh or complicated dissection
of the inguinal floor as in Bassini/Shouldice. It has shown excellent results
with virtually zero recurrence rates.
KEY WORDS: Inguinal hernia,
Herniorrhaphy, Physiological repair, Recurrence
INTRODUCTION
An editorial in Annals of
Surgery, January 2001, raised the question of whether the changed
techniques of hernia repair in recent years, mainly implanted mesh, have caused
a rise in the incidence of chronic groin pain from 1% to 28.7% after hernia
repairs. The recurrence rate after hernia repair done by expert surgeons is
less than 2%, but in the hands of junior surgeons, it is still much higher [2,3].
The problem of our age is to find an operation that is simple, does not require
implantation of a foreign body like mesh, has a recurrence rate of less than
1-2% and does not produce major complications during or after surgery in the
hands of non-consultant staff. Nicholson, in his leading article on inguinal
hernia repair in British Journal of Surgery (1999) states that:
"With over 80 000 groin hernia operations carried out in the UK alone
each year, and a deepening crisis in surgical manpower resulting from increased
surgical sub specialization and greater public and political demands for
quality in surgical practice, inguinal hernia repair will remain for the
foreseeable future a procedure likely to be delegated to non-consultant staff.
It is essential therefore that we design safe and simple pathways for managing
these patients."
The
author’s technique seems to provide such a hernia repair. It is based on the
concept of providing a strong, mobile, and physiologically dynamic posterior
wall. The present study is conducted to show the results of a larger series of
860 patients with follow up of more than 7 years. This series includes only 220
patients of the previously published series.
PATIENTS
AND METHODS
860 patients having 920 inguinal
hernias, between 18 to 90 years of age (mean age 50.5 years), were operated on
between August1990 and December 2003. Patients were not selected in any way and
all the patients admitted under the care of the author for hernia repair were
operated by this technique. 549 patients were operated on under spinal
anaesthesia, 302 under local anaesthesia and 9 had a general anesthetic.
Sutures were removed on the eighth day. Ampiclox (ampicillin and cloxacillin)
and diclofanac were given for a week due to social and hygienic conditions at
home. Pain, ambulation and return to normal activities were assessed by using
the Short Form 36 questionnaire and a visual analog scale. Pain was described
as none, mild, moderate, severe and very severe. Movements from bed to bathroom
inside the room were termed as limited movements and movements outside of the
room were termed as free movements. The author followed up patients personally
at 15 days, 1, 3 months, and later every year. 598 patients attended the clinic
for follow up for 7 years. Appearance of a bulge in the groin on coughing was
treated as a recurrence, which was confirmed by clinical examination. A
questionnaire was sent to 25 patients who could not attend the clinic for
follow up regularly or left the follow up in between.
OPERATIVE TECHNIQUE: A regular
oblique inguinal incision is taken. The EOA is cut to open the inguinal canal.
Herniotomy is done as usual and the hernia sac is inverted or excised. The
medial leaf of the EOA is sutured to the inguinal ligament from the pubic
tubercle to the abdominal ring using 1/0 polypropylene interrupted sutures. The
first 1-2 sutures are taken in the anterior rectus sheath. The last suture is
taken so as to narrow the abdominal ring sufficiently without constricting the
spermatic cord (Fig.1).
FIG.1. Medial leaf of EOA is sutured to the
inguinal ligament with splitting incision taken
1=Medial leaf; 2=Continuous absorbable sutures
taken to suture the medial leaf to the inguinal ligament; 3=Pubic tubercle;
4=Abdominal ring; 5=Spermatic cord; 6= Lateral leaf.
A splitting incision is made in this sutured medial leaf,
partially separating a strip of a width of 1.5 to 2 cms. This splitting
incision is extended medially up to the rectus sheath and laterally 1-2 cms
beyond the abdominal ring. The medial insertion and lateral continuation of
this strip is kept intact. A strip of the EOA, is now available, the lower border
of which is already sutured to the inguinal ligament. The upper free border of
the strip is now sutured to the internal oblique or muscle arch lying close to
it with 1/0 polypropylene interrupted sutures throughout its length (Fig.2).
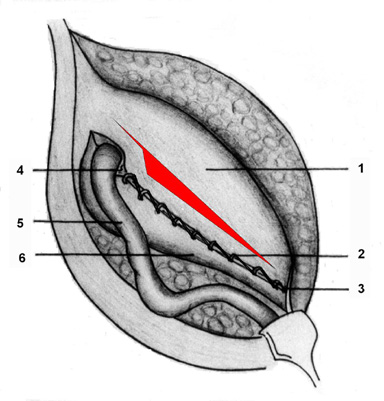
FIG.2. Undetached strip of external oblique
aponeurosis forming the posterior wall of inguinal canal.1=Reflected medial
leaf after a strip has been separated; 2= Internal oblique muscle seen through
the splitting incision made in the medial leaf; 3= Continuous absorbable
sutures between the upper border of the strip and conjoined muscle or internal
oblique muscle; 4= Continuous absorbable sutures between the lower border of
the strip and the inguinal ligament; 5=Pubic tubercle; 6= Abdominal ring;
7=Spermatic cord; and 8= Lateral leaf.
The aponeurotic portion of the internal oblique muscle is used
for suturing to this strip wherever and whenever possible without tension;
otherwise, it is not a must for the success of the operation. This will result
in the strip of the EOA being placed behind the cord to form a new posterior
wall of the inguinal canal. At this stage the patient is asked to cough and the
increased tension in the strip is clearly visible. The spermatic cord is placed
in the inguinal canal and the lateral leaf of the EOA is sutured to the newly
formed medial leaf of the EOA in front of the cord, as usual, again using 1/0
polypropylene interrupted sutures. Undermining of the newly formed medial leaf
on both of its surfaces and excision of the bulky cremasteric muscle (if
required) facilitates its approximation to the lateral leaf without tension.
The first stitch is taken between the lateral corner of the splitting incision
and lateral leaf of the EOA. This is followed by closure of the superficial
fascia and the skin as usual.
RESULTS
Inguinal hernia was indirect in
44.35 % of cases (408 patients), direct in 34.57 % (318 patients, pantaloon
(mixed) type in 0.65 % (6 patients), obstructed in 3.48% (32 patients) and
recurrent in 16.95% cases(156 patients). 792(92%) patients required a stay of
18-24 hours, 60(7%) for 24-48 hours and 8 (1%) stayed for more than 48 hours.
845(98.25%) patients were ambulatory with limited movements up to bathroom
within 6-8 hours and had free movements within 18-24 hours. 840(97.6%) of patients
returned to normal activities like bending, kneeling, or stooping, climbing one
or more flights of stairs, carrying groceries or attending office duties or
doing normal routine pre-operative non vigorous activities within 4-14 days. 620 (72%) patients had mild pain locally for 2 days, 206 (24%)
for 4 days and 34 (4%) patients had mild pain for 7-15 days. No patient had
severe or very severe pain. Seven patients had wound oedema during the
postoperative period which subsided on its own. Five patients had mild skin
infection and one patient had Haematoma that was drained. A total of 860 (100%)
returned for a follow up visit after 15 days and one month; 847 (98.5%) for 3
months; 752 (87.5%) for 1 year; 683 (79.4%) for 3 years and 623 (72.5%)
patients were followed up for more than 7 years. The median follow up period
was 7.8 years. There were no recurrences or late complications. It was observed
that the aponeurotic extensions from the transverses abdominis aponeurotic arch
were absent or deficient and the posterior wall was weak and flabby in all the
patients. The aponeurotic strip of the EOA gave a strong and physiologically
dynamic posterior wall in all these patients. 99% of patients operated under
local or low epidural anesthesia showed dynamic nature of the strip when the
patient was asked to cough on the operation table. It was also observed that
the muscle arch, which was inactive or less active, showed good movements or
improved movements after the repair was done. This was obviously due to the new
anchorage to the inguinal ligament it received through the strip.
DISCUSSION
The transversalis fascia acts as a
barrier to prevent hernia because it is supported in the posterior wall by
aponeurotic extensions from the muscle arch. The transversalis fascia alone
cannot withstand the raised intra-abdominal pressure for a longer period if the
aponeurotic element in the posterior wall is absent or deficient. Strong
musculo-aponeurotic structures around the inguinal canal still give protection
to prevent the herniation in such individuals. This protection is lost if those
muscles are weak. The weak and physiologically adynamic posterior wall of
inguinal canal in such individuals leads to hernia formation [4]. Therefore,
the aim of hernia repair should be to provide a strong, mobile, and
physiologically dynamic posterior wall.
Bassini, Halsted, McVay, and
Shouldice had advised excision of the transversalis fascia requiring extensive
dissection. Amid et al [5] reported that to use already weakened
muscles and transversalis fascia, particularly under tension, is a violation of
the most basic principles of surgery. Weak muscles used in those repairs fail
to give a strong and physiologically dynamic posterior wall. Hay et al [6]
compared the Shouldice to the Bassini and Cooper’s ligament repair and found in
a study of 1578 hernias with a mean follow up of 8.5 years, a recurrence rate
of 6 % compared with Bassini 8.6 %, and Cooper’s ligament repair 11 %. Panos et
al [7] and Kingsnorth et al [2] stated that the reported
recurrence rates from smaller hospitals seem to be worse than those from
specialist centers. The operation described by Lichtenstein is simple and safe.
But the mesh prosthesis has its drawbacks. The slightest movement of the mesh
from the sutured area is a leading cause of failure of mesh repair of inguinal
hernias [8]. Mesh works as a mechanical barrier. It does not give
mobile and physiologically dynamic posterior wall.
The
aging process is minimum in the tendons and aponeurosis, so a strip of the
external oblique, which is tendo-aponeurotic, is the best alternative to the
mesh. The author has used the thinned out portion of the external oblique with
good results.
Double breasting of EOA was
described by Zimmerman for repairs of inguinal hernias [9]. In
Andrew’s imbrications operation (Wyllys Andrews operation, Chicago Med. Rec. N
Y 9:67, 1895), the entire medial leaf of the external oblique together with the
muscle arch is sutured to the inguinal ligament and the lateral leaf is used to
cover the cord in front. The author’s operation differs from the Andrew’s
technique because the procedure of strengthening the posterior wall of the
inguinal canal is different and the mechanism of action involved is also
different.
MECHANISM OF ACTION: Contraction of
the external oblique muscle creates lateral tension in this strip while
contraction of the internal oblique / conjoined muscle pulls this strip upwards
and laterally creating tension above and laterally, making the strip a shield
to prevent any herniation. This additional strength given by the external
oblique muscle to the weakened conjoined muscle to create tension in the strip
and prevent reherniation is the essence of this operation. Tension created in this
strip is graded as per the force of muscle contractions. Stronger
intra-abdominal blows result in stronger abdominal muscle contractions and
stronger muscle contractions result in increased tension in this strip to give
graded protection. The strip or the suture line is without any tension at rest.
Thus, a strong and physiologically dynamic posterior wall is prepared in this
operation.
CONCLUSIONS: The author’s technique
is simple and easy to do and learn. It does not require complicated dissection
or suturing. There is no tension on the suture line. It does not require any
foreign material and does not use weakened muscles or transversalis fascia for
repair. The results are superior to those previously published in the field of
hernia surgery. This prospective cohort study is conducted by the author alone
and therefore may be subject to a personal bias.
PERSONAL COMMUNICATION: Since its
first publication in 2001, the author received communication from the following
surgeons in Poland, Cuba, Korea, Albania and India of clinical trials being
conducted by them that had shown similar results without recurrence till date.
1] Collegium Medicum in Bydgoszcz, Nicolaus Copernicus University
(Department of General
and
Endocrine Surgery), ul.M.Sk³odowskiej-Curie 9, 85-096 BYDGOSZCZ, POLAND
Contact: Jacek SZopinski, M.D
(Professor of Surgery); Email: jacek.szopinski@wp.pl
2] Hospital General Docente Enrique
Cabrera. (Department of General Surgery)
Calle Aldabo No. 11117. Altahabana.
Municipio Boyeros. Ciudad Habana, Cuba.
Contact: Pedro Lopez (Professor of
Surgery); Email: lopezp@infomed.sld.cu,
3] B.J.Medical College and Sassoon
General Hospital, (Department of surgery), Pune- 411001,
India, Contact: Sudhir Dube
(Professor of surgery); Email: drdubesb@yahoo.co.in,
4]
Contact: Kishik Kye, M.D.; Email:
kskye@hanafos.com,
5] Civil Hospital. City of
Contact: Robert Metaj, M.D. (Chief
surgeon); Email: metajrobert@yahoo.com,
6] Surgeons working in different
medical institutions in many cities of India, like Calcutta, Chennai, Sholapur,
Dhavangiri, Kanpur, Karad, Meerut, Belgaum, Baroda, Nanded etc. had conducted
trials of this technique for thesis purposes of their post graduate students.
Following surgeons from different
countries communicated and showed interest in this technique but there was no
follow up communication later and the contact is lost.
1] J.
Olejnik, Chirurgika Klinika, FN Akad. Derera,
Limbova 5; 833 05 Brtislava (Slovakia), 2] Cornelius Lemke,Friedrich Schiller
University, Institute of Anatomy, D-07740 Jena, Germany, 3] Dr. Y. Bayon,
Sofradim production, 116 Avenue Du Formans , 01600 Trevoux, France, 4] Peter
Bruncak,M.D. District Hospital, Nam, Republiky 14, 984 39 Lucenec (Slovakia),
5] Dr. Abel Santana, Gonzalez-Chavez, EMAIL: abel@ventila.mtz.sld.cu, 6]
R.Elamiyal, Al-Arab Medical University, Benghazi, Libiya, 7] Filipe Delgado,
Hospital Pediatrico Docente "Willium Soler" Apartado No. 8019,
Habana-8, Cuba, 8] Miller Junny, EMAIL: MILLERJUNNY@cs.com ,
REFERENCES
1.
Desarda
MP (2001) New method of inguinal hernia repair-A new solution. ANZ J Surg
71:241-44.
2.
Kingsnorth
AN, Gray MR, Nott DM (1992) Prospective randomized trial comparing the
Shouldice technique and plication darn for inguinal hernia. Br J Surg 79:
1068-1070.
3.
Kux
M, Fuchsjager N, Schemper M (1994) Shouldice is superior to Bassini inguinal
herniorrhaphy. Am J Surg 168: 15-18.
4.
Desarda
MP (2003) Surgical physiology of inguinal hernia repair-A study of 200 cases.
BMC Surgery 3:2.
5.
Amid
PK, Shulman AG, Lichtenstein L (1991) Femoral hernia resulting from inguinal
herniorrhaphy - the ‘plug’ repair. Contemp Surg 39: 19-24.
6.
Hay JM,
Boudet MJ, Fingerhut A et al (1995) Shouldice inguinal hernia repair in the
male adult: the gold standard? A multicentre controlled trial in 1578 patients.
Ann Surg 222: 719-727.
7.
Panos
RG, Beck DE, Maresh JN, Harford FJ (1992) Preliminary results of a prospective
randomized study of Cooper’s ligament vs Shouldice herniorrhaphy technique Surg
Gynecol Obstet 175: 315-319.
8.
Amid
PK,
9. Zimmerman LM (1952) Recent advances in
surgery of inguinal hernia. Surg Clin North Am 32: 135-154.
{kind=link}
{kind=link}