|
WE INVITE YOUR COMMENTS
|

|

HOME |
PAPERS |
NEWSLETTER |
|
|
Based on the Windana Experience WFTC 21st World Conference, Carlton Crest, Melbourne, Australia 17th-22nd February, 2002 |
|
|
|
Dr. Barbara Brewitt, (1997) M Div, PhD, Biomed Comm, Inc., Seattle planned and
conducted a Reiki research project with chronically ill clients.
Five patients with illnesses of multiple sclerosis, MS(n=2), lupus,
fibromyalgia, or thyroid goitre were given eleven one-hour Reiki sessions using
four different Reiki Level Two practitioners and one Reiki master over a
ten-week time period. There were three measurements per person of electrical
skin resistance on the hands and feet of patients in the Reiki Study.
Out of the forty-five skin points measured, three points showed significant
difference during and after Reiki sessions. All patients made written comments
regarding increased relaxation or sense of "centeredness" after Reiki sessions.
All patients reported to practitioners that there was a reduction in pain and
an increase in mobility.
We refer to these studies to support our claim that giving Reiki induces more
than a placebo response in clients. In our experience, it seems to have
physical, emotional and even spiritual effects during the treatment and post
treatment phases, which we will illustrate more clearly when discussing our
experience in the Reiki clinic.
During Reiki treatment, the energy is not manipulated or modified by the
practitioner. Rather the practitioner, who has been attuned to the energy, is
a conduit through whom the energy flows to the receiver as soon as the
practitioner's hands are placed on the recipient's body or enter their energy
fields.
Empirical evidence indicates that the receiver cannot receive too much Reiki
energy as the flow ceases once sufficient has been transmitted. Both giver and
receiver of Reiki are often aware of this automatic switching on and off, of
the energy flow.
REIKI TREATMENT AT WINDANA
In that time, approximately fourteen hundred treatments have been given to
residents in the program at the Reiki Clinic. The Clinic, which is conducted
with professional guidelines, is overseen by a paid supervisor who coordinates
a team of volunteers. Treatment records are kept and after each session, a
debriefing is held and a handover made to staff in the DWH.
The two forms of Reiki treatment practiced in the Clinic are Reiki Jin Kei Do
(the traditional eastern method) and the Usui System of Reiki Healing (the
system originally brought to the West). Both stem from the teachings of Mikao
Usui, although Reiki Jin Kei Do has more direct linkage to the origins of Reiki
practice in Nepal and the Himalayas.
The importance of practising according to a form will be dealt with in the
Workshop on the Reiki Clinic at Windana, later in this (paper).
Since its inception, the Clinic has, apart from being the source of the 1995
paper mentioned above, also been the inspiration for the creation of a Reiki
Practitioner Development Course and the establishment of the professional Reiki
association, 'Reiki Association of Practitioners and Masters Inc.' (RAPMA). The
RAPMA Practitioner Codes of Ethics and Practice were largely informed by the
observed needs for professionalism in the Reiki Clinic.
Originally the Clinic operated informally with clients from the general
community. In the early stages residents of the DWH were offered treatments
only when there were free treatment times available.
It was soon noticed, by those undergoing withdrawal, that Reiki appeared to
have significant benefits, and more residents began to volunteer for Reiki
treatments. DWH staff, noticing the benefits that clients appeared to have
from receiving Reiki, began to actively encourage the clients to attend the
Clinic.
The Reiki Clinic is now an integral part, along with other natural therapies,
of the DWH program.
The majority of the clients residing in the DWH, at first contact, know little
or nothing of Reiki and therefore have no expectations. Quite a few declare
themselves to be skeptical and even at times, apprehensive. The latter often
report great surprise at the depth of relaxation felt.
As previously stated, given the scarcity of research on Reiki in general and
specifically in relation to the area of drug and alcohol withdrawal and
rehabilitation programs, we have had to rely on the empirical evidence of the
effects of Reiki reported by clients post treatment.
However, client records taken in the nine and a half years of the Clinic's
operation indicate some very clear themes of the effects of Reiki on those DWH
residents who have come for treatment. These themes are supported by a recent
survey of DWH staff.
The main themes consistently identified from clinic records, as reported by DWH
residents, were improvement in:
A small survey of staff at the residential community at Windana, assessed staff
views of the response of residents to Reiki treatment. A 10cm Likert scale was
used. Eight questionnaires were returned. (5 from female staff, and 3 from
male staff). Five of the staff had personally experienced Reiki.
Their comments included:
Given comments from residents about Reiki over the last 9 years, we decided to
address the 8 main treatment outcomes in the staff questionnaire (that we had
identified from the residents' responses.
The first was staff observation of behaviour change in residents following
Reiki treatment.
This indicates that about half the staff noticed an improvement in the residents' behaviour after treatment.
Their comments included:
Comments included:
Many of the staff were unsure, or unable to comment about any changes in the residents sleep pattern, because of the times they are in contact with them. However, there were some responses to this question.
In relation to an improvement in the residents relaxation, communication and
clarity of thought after Reiki, there was a strong perception that Reiki had a
relaxing effect, but more uncertainty about improvement in communication and
clarity of thought.

In reference to relaxation, staff made comments such as:
Regarding communication and clarity of thought, only the following two comments
were made:
Many staff were unsure about the questions:
Their responses were as follows:

We asked these two questions because these outcomes have frequently been
attributed to the Reiki treatment over the 9 years of clinic operation, by both
residents and staff.
It is interesting that improvement is not reflected in the staff responses.
However improvement in insight by residents was a consistent factor in their
comments at the Reiki clinic, and this will be illustrated later in this paper.
The last question we asked was staff perception of improvement in the
residents' feelings about the rehabilitation program and of life in general,
after having Reiki treatment.
Again, it was difficult for staff to comment about any one treatment in all the
therapies offered by Windana. However, their responses were generally positive,
as shown in the next graph:
As practitioners at the clinic, we believe that after a Reiki treatment we
often see the person as we believe they more truly are. More importantly, they
themselves appear to experience or begin to experience who they are.
A staff member made the observation that this experience provides the
possibility for change because they are released from the self perception of
victim-hood and begin to see themselves as a person, who happens to have a drug
habit or addiction, rather than saying to themselves,
"I am a drug addict - or alcoholic."
A clinical psychologist, who visited the clinic twice to observe, commented
that:
"The Reiki treatment appears to permit a profound shift in awareness to occur
which allows clients to connect with aspects of self (mind and body) normally
not freely accessible and in so doing, offers the potential for meaningful
self-understanding to emerge. Integrally associated are relaxation, comfort and
ease"
(Alexander, in Chapman 1996).
Alexander goes on to say that there are a number of other clinical techniques
and methods which would similarly re-create emotional and memory connections,
previously out of awareness; such as hypnosis and Gendlin's Focusing (1981).
In this respect, however, it is interesting to note that Reiki, unlike other
clinical techniques, creates altered states spontaneously, without intervention
by the practitioner (other than routine hand placement).
Obviously, therefore, the pain relief experienced by many of the people in
detox is a contributing factor in enabling them to stay in the programme and to
make positive choices for their future.
Many of the clients in the DWH program are so used to having pain that they do
not mention it when presenting for treatment and simply report, with surprise,
that the pain has either lessened or gone completely. All who report with pain
report some pain relief.
One DWH client reported that the pain he had been experiencing in his arm
following a recent operation and which, according to him had been "driving me
mad", had eased considerably. Others experience relief from the aches, pains
and physical spasms of withdrawal.
Sometimes the pain is relieved in an area which has not had hand contact from
the practitioner, as illustrated in the following case study.
After treatment, he reported the sensation of energy travelling from where the
practitioner's hands were placed on his chest, to his hip which he said was
almost always painful due to arthritis, resultant from a road accident some
years previously.
He said that "the energy created an increasing sensation of pain in my hip
which became almost intolerable and then gradually subsided".
When asked how his hip was feeling after the treatment he said that it was pain
free. As this was a chronic condition, it was explained to him that the pain
could re-occur.
When we saw him again some weeks later, he told us that the pain had indeed
returned - but never to the degree that it had been prior to his previous Reiki
treatment.
We invite comment on the content and direction of this paper from practitioners of Reiki who either are already working, or are contemplating working in the professional field, such as in hospital, hospice, or clinic situations. We are also creating a dossier of case studies dealing with the effects of psychic practice in Reiki - both harmful or otherwise - and will appreciate the receipt in writing of any relevant case studies. We would stress that confidentially will be maintained in these case studies: where appropriate, names of persons involved will be omitted or changed. |



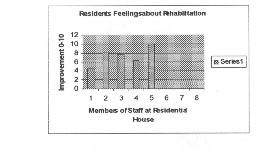 Fig. 9. Perceptions about residents' feelings about rehabilitation.
Fig. 9. Perceptions about residents' feelings about rehabilitation.
|
Mornington Peninsula Reiki Centre, PO Box 17, Bittern, 3918. Phone/Fax (03) 5983 9971. |
Reiki Journey Centre, Clifton Hill, 3068, Phone/Fax (03) 9482 5336. |
|
|