Transmission
Smallpox
Definition
Smallpox was a highly contageous human disease caused by the virus viriolae. There are two strains: viriole major, which had severe symptoms and a very high mortality (20-40%), and viriole minor, which had less severe symptoms and lower mortality (about 1%). The disease most commonly confused with smallpox is chickenpox, and during the first 2 to 3 days of rash, it may be all but impossible to distinguish between the two. However, all smallpox lesions develop at the same pace and, on any part of the body, appear identical. Chickenpox lesions are much more superficial and develop in crops. With chickenpox, scabs, vesicles, and pustules may be seen simultaneously on adjacent areas of skin. Moreover, the rash in chickenpox is more dense over the trunk (the reverse of smallpox), and chickenpox lesions are almost never found on the palms or soles. In 5% to 10% of smallpox patients, more rapidly progressive, malignant disease develops, which is almost always fatal within 5 to 7 days. In such patients, the lesions are so densely confluent that the skin looks like crepe rubber; some patients exhibit bleeding into the skin and intestinal tract. Such cases are difficult to diagnose, but they are exceedingly infectious.
Symptoms
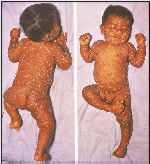
Smallpox is characterised in its classical form by the sudden onset of fever, headache, backache, vomiting, marked prostration and even delirium. At this early stage the patient may be very ill and compelled to take to his bed. Early in the illness there may appear in about 10% of patients a fleeting rash in the form of a reddening of the skin, not unlike the rash of German Measles. This is the so-called prodromal rash and, in the absence of a history of exposure to a source of infection, there is nothing about htis rash to arouse suspicion of smallpox. The incubation period from exposure to the onset of this feverish illness is nearly always 12 days with very little variation either way. About two to three days after the onset of illness the true smallpox rash appears. At this time any prodromal rash will be fading. This true or so-called focal rash is normally diagnostic of smallpox and is characteristic both in its evolution and distribution on the body. It begins as tiny discrete pink spots, macules, which enlarge and become slightly raised papules. Each of these progresses by the third day to become a tense blister, vesicle, 6mm in diameter, deep in the skin. After two more days the fluid inside becomes turbid and the lesions are not described as pustules or by the older term of pocks. In the following days these shrink and dry up to become hard lentil-like crusts ni the skin. Eventually they separate leaving a sunken scar. The hard material which comes away contains smallpox virus in its substance. The distribution of this focal rash is characteristic, affecting the head and extremeties much more than the trunk. These features make classical smallpox easy to diagnose clinically when once the thought of the disease has entered the mind. There is some correlation between severity of illness and extent of focal rash. Toxaemia may be so sever as to cause death even before the rash is fully developed, but more commonly death, if it ocurs, will be between the 11th and 15th day of the rash. In severe cases the rash may cover the entire body and the individual lesions run into one anotehr to become confluent.
Transmission
A person infected with smallpox and overtly sick usually transmits the virus face-to-face in a closed dwelling. There is no infectious subclinical state.
Diagnosis
Great diagnostic difficulties arise through wide variations from this characteristic pattern. Very severe disease may result in death even before the focal rash is fully developed and sometimes, as in haemorrhagic smallpox bleeding into the skin and from the body orifices wrongly focuses attention towards some severe and acute blood disease.
Treatment
The only weapons against the disease are vaccination and patient isolation. Smallpox vaccination is NOT available for the genertal public Vaccination before exposure or within 2 to 3 days after exposure affords almost complete protection against disease. Vaccination as late as 4 to 5 days after exposure may protect against death. Because smallpox can only be transmitted from the time of the earliest appearance of rash, early detection of cases and prompt vaccination of all contacts is critical. Smallpox vaccination is associated with some risk for adverse reactions; the two most serious are postvaccinal encephalitis and progressive vaccinia. Postvaccinal encephalitis occurs at a rate of 3 per million primary vaccinees; 40% of the cases are fatal, and some patients are left with permanent neurologic damage. Progressive vaccinia occurs among those who are immunosuppressed because of a congenital defect, malignancy, radiation therapy, or AIDS. The vaccinia virus simply continues to grow, and unless these patients are treated with vaccinia immune globulin, they may not recover. Pustular material from the vaccination site may also be transferred to other parts of the body, sometimes with serious results. Routine vaccination is only recommended for laboratory staff who may be exposed to one of the orthopoxviruses. There are two reasons for this. First is the risk for complications. Second, U.S. national vaccine stocks are sufficient to immunize only 6 to 7 million persons. This amount is only marginally sufficient for emergency needs. Plans are now being made to expand this reserve. However, at least 36 months are required before large quantities can be produced.
Prevention
The only weapons against the disease are vaccination and patient isolation. Smallpox vaccination is NOT available for the genertal public Vaccination before exposure or within 2 to 3 days after exposure affords almost complete protection against disease. Vaccination as late as 4 to 5 days after exposure may protect against death. Second, U.S. national vaccine stocks are sufficient to immunize only 6 to 7 million persons. This amount is only marginally sufficient for emergency needs. Plans are now being made to expand this reserve. However, at least 36 months are required before large quantities can be produced.

Links
Protection from Chemical Hazards
Wildpony ..... The Druidess Casts Her Spell
Biological Agents:
Anthrax/Botulism/Brucellosis/Campylobacteriosis/Cholera/Dengue Fever/Ebola Fever/E. Coli/Hanta Fever/Lassa Hemorrhagic Fever/Legionellosis/Marburg Hemorrhagic Fever/ Plague/Rift Valley Fever/Smallpox/Streptococcus/Tularemia/West Nile Fever
